Download præsentationen
Præsentation er lastning. Vent venligst

1
Reumatoid artrit og Kardiovaskulær sygdom Rekommendationer
Ulrik Tarp Lektor, overlæge, dr.med. Reumatologisk afdeling Århus Universitetshospital

2
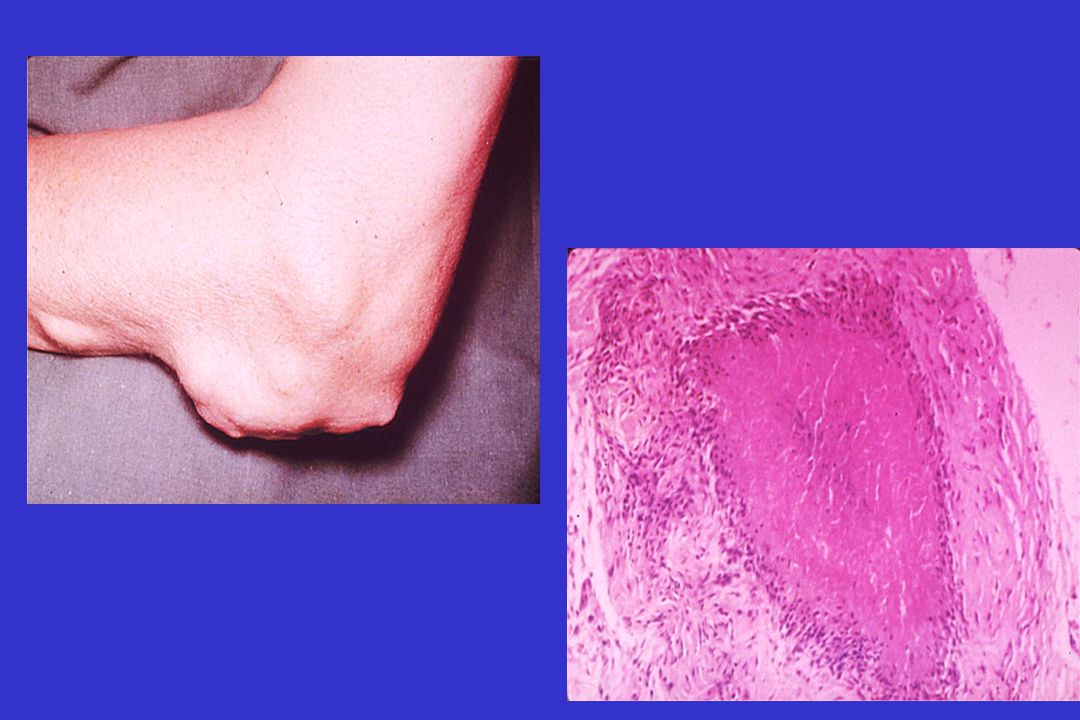
Normal vs. Rheumatoid Synovium
Normal synovium 1-cell-layer thick Few blood vessels No inflammatory cells Rheumatoid synovium—pathologic alterations Synovial hyperplasia Inflammatory infiltrate (major infiltration of leukocytes and other inflammatory cells) Increased vascularity Normal synovium Rheumatoid synovium Koopman WJ, ed.: Arthritis and Allied Conditions, 14th ed., Copyright © 2001 Lippincott, Williams & Wilkins
 Increased vascularity. Normal synovium Rheumatoid synovium. Koopman WJ, ed.: Arthritis and Allied Conditions, 14th ed., Copyright © 2001 Lippincott, Williams & Wilkins.")
4
Epidemiologi Afficerer ca. 0.5–1% af befolkningen
Estimeret årlig incidens Mænd: 0.1–0.2 per 1000 Kvinder: 0.2–0.4 per 1000 2 til 3 gange hyppigere hos kvinder end mænd Rammer alle aldre Hyppigst mellem 45 og 65 år RA affects about 1% of the population.1 The annual incidence of RA is estimated to be 0.1 to 0.2 per 1000 in males and 0.2 to 0.4 per 1000 in females.2 The incidence and prevalence of RA are 2 to 3 times higher in women than in men.1 The disease has been found around the world in many different races and cultures.2 The peak age of onset of RA is between 45 and 65 years.2 Sangha O. Rheumatology. 2000;39(suppl 2):3–12. MacGregor AJ, Silman AJ. In: Klippel JH, Dieppe PA, eds. Rheumatology. Vol 1. 2nd ed. London, England: Mosby; 1998:2.1–2.6. 1. Sangha O. Epidemiology of rheumatic diseases. Rheumatology. 2000;39(suppl 2):3-12. 2. MacGregor AJ, Silman AJ. Classification and epidemiology. In: Klippel JH, Dieppe PA, eds. Rheumatology. Vol 1. 2nd ed. London, UK: Mosby; 1998: Page 4
:3–12. MacGregor AJ, Silman AJ. In: Klippel JH, Dieppe PA, eds. Rheumatology. Vol 1. 2nd ed. London, England: Mosby; 1998:2.1– Sangha O. Epidemiology of rheumatic diseases. Rheumatology. 2000;39(suppl 2): MacGregor AJ, Silman AJ. Classification and epidemiology. In: Klippel JH, Dieppe PA, eds. Rheumatology. Vol 1. 2nd ed. London, UK: Mosby; 1998: Page 4.")
5
Clinical Features of RA
These are the recognizable hands of a patient with active RA. Here you see the typical changes in the hand, including swelling of the MCPs and PIPs. (PIPs = proximal interphalangeal joints) We know at least one thing for sure with RA—once a patient has it, it will only get worse. What we don’t know with a very high degree of confidence is when, how much and how fast it will get worse.
 We know at least one thing for sure with RA—once a patient has it, it will only get worse. What we don’t know with a very high degree of confidence is when, how much and how fast it will get worse.")
6
Clinical Features of RA
Typical changes in hands of RA patient: Pannus formation in MCPs, PIPs and wrists

7
Radiologic Features Early/intermediate stage Soft tissue swelling
Mild juxta-articular osteoporosis Narrowing of joint space Bone erosions Early in the course of RA, soft tissue swelling may be the only radiographic sign of disease.1 During the intermediate stage of the disease, signs include mild juxtaarticular osteoporosis, narrowing of the joint space (from cartilage loss), and bone erosions.1,2 Early radiographic joint damage is predictive of aggressive further development of RA. In late-stage RA, radiographs can reveal large erosions, anatomic deformities, and ankylosis.1 Initially, RA usually affects the ulnar styloid, I-III metacarpophalangeal joints, and II-III proximal interphalangeal joints.2 The most common extraarticular lesions are subcutaneous nodules, usually appearing on the extensor surfaces of the arms and elbows. Other imaging techniques (e.g., ultrasound of the affected joint, computed axial tomography, magnetic resonance imaging) can be helpful in assessing the features of a patient’s disease and the extent of anatomic damage.2 Early erosions in the “bare” areas of the second and fourth metacarpal heads in RA. The erosions are the disruption of continuity of the white cortical line arrows. Brower AC. In: Klippel JH, Dieppe PA, eds. Rheumatology. Vol 1. 2nd ed. Philadelphia, Pa: WB Saunders; 1998;5:5.1–5.8. Resnick D et al. In: Kelley WN et al, eds. Textbook of Rheumatology. 5th ed. Philadelphia, Pa: WB Saunders; 1997:626–685. 1. Resnick D, Yu JS, Sartoris D. Imaging. In: Kelley WN, Harris ED Jr, Ruddy S, et al, eds.Textbook of Rheumatology. 5th ed. Philadelphia, PA: WB Saunders; 1997: 2. Grassi W, De Angelis R, Lamanna G, Cervini C. The clinical features of rheumatoid arthritis. Eur J Radiol. 1998;27(suppl 1):S18-S24.
, and bone erosions.1,2 Early radiographic joint damage is predictive of aggressive further development of RA. In late-stage RA, radiographs can reveal large erosions, anatomic deformities, and ankylosis.1. Initially, RA usually affects the ulnar styloid, I-III metacarpophalangeal joints, and II-III proximal interphalangeal joints.2. The most common extraarticular lesions are subcutaneous nodules, usually appearing on the extensor surfaces of the arms and elbows. Other imaging techniques (e.g., ultrasound of the affected joint, computed axial tomography, magnetic resonance imaging) can be helpful in assessing the features of a patient’s disease and the extent of anatomic damage.2. Early erosions in the bare areas of the second and fourth metacarpal heads in RA. The erosions are the disruption of continuity of the white cortical line arrows. Brower AC. In: Klippel JH, Dieppe PA, eds. Rheumatology. Vol 1. 2nd ed. Philadelphia, Pa: WB Saunders; 1998;5:5.1–5.8. Resnick D et al. In: Kelley WN et al, eds. Textbook of Rheumatology. 5th ed. Philadelphia, Pa: WB Saunders; 1997:626– Resnick D, Yu JS, Sartoris D. Imaging. In: Kelley WN, Harris ED Jr, Ruddy S, et al, eds.Textbook of Rheumatology. 5th ed. Philadelphia, PA: WB Saunders; 1997: Grassi W, De Angelis R, Lamanna G, Cervini C. The clinical features of rheumatoid arthritis. Eur J Radiol. 1998;27(suppl 1):S18-S24.")
8
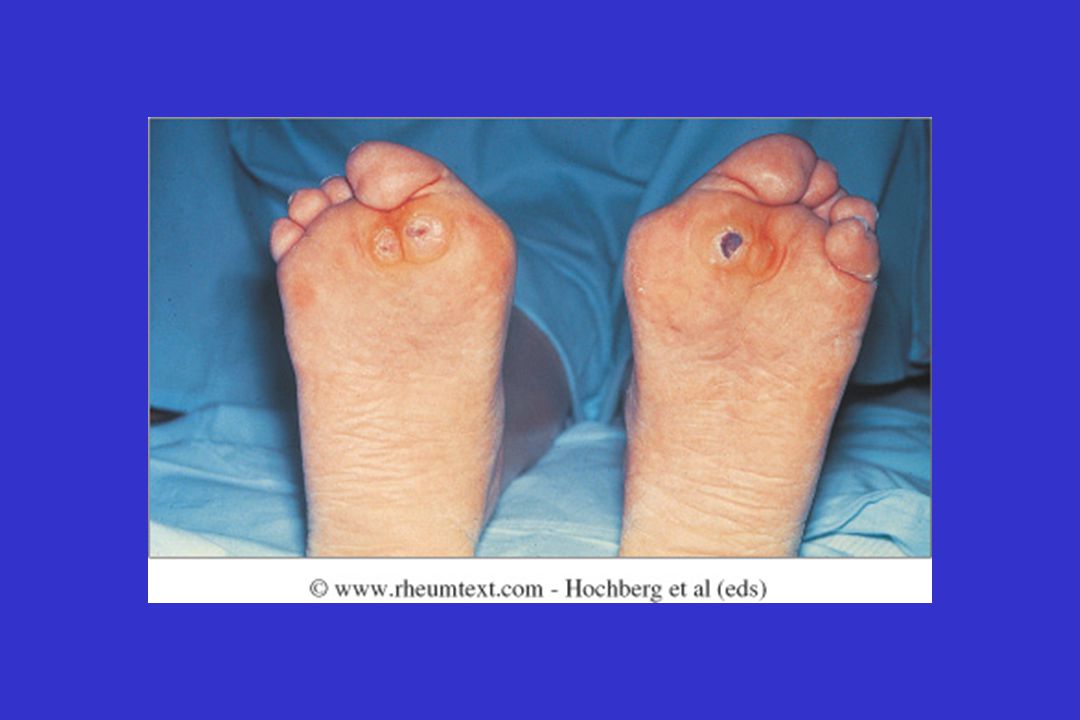
Radiologic Features Late stage
Large erosions, anatomic deformities, ankylosis Complete loss of joint spaces and heads of MTPs Early in the course of RA, soft tissue swelling may be the only radiographic sign of disease.1 During the intermediate stage of the disease, signs include mild juxtaarticular osteoporosis, narrowing of the joint space (from cartilage loss), and bone erosions.1,2 Early radiographic joint damage is predictive of aggressive further development of RA. In late-stage RA, radiographs can reveal large erosions, anatomic deformities, and ankylosis.1 Initially, RA usually affects the ulnar styloid, I-III metacarpophalangeal joints, and II-III proximal interphalangeal joints.2 The most common extra-articular lesions are subcutaneous nodules, usually appearing on the extensor surfaces of the arms and elbows. Other imaging techniques (e.g., ultrasound of the affected joint, computed axial tomography, magnetic resonance imaging) can be helpful in assessing the features of a patient’s disease and the extent of anatomic damage.2 Brower AC. In: Klippel JH, Dieppe PA, eds. Rheumatology. Vol 1. 2nd ed. Philadelphia, Pa: WB Saunders; 1998;5:5.1–5.8. Resnick D et al. In: Kelley WN et al, eds. Textbook of Rheumatology. 5th ed. Philadelphia, Pa: WB Saunders; 1997:626–685. 1. Resnick D, Yu JS, Sartoris D. Imaging. In: Kelley WN, Harris ED Jr, Ruddy S, et al, eds.Textbook of Rheumatology. 5th ed. Philadelphia, PA: WB Saunders; 1997: 2. Grassi W, De Angelis R, Lamanna G, Cervini C. The clinical features of rheumatoid arthritis. Eur J Radiol. 1998;27(suppl 1):S18-S24.
, and bone erosions.1,2 Early radiographic joint damage is predictive of aggressive further development of RA. In late-stage RA, radiographs can reveal large erosions, anatomic deformities, and ankylosis.1. Initially, RA usually affects the ulnar styloid, I-III metacarpophalangeal joints, and II-III proximal interphalangeal joints.2. The most common extra-articular lesions are subcutaneous nodules, usually appearing on the extensor surfaces of the arms and elbows. Other imaging techniques (e.g., ultrasound of the affected joint, computed axial tomography, magnetic resonance imaging) can be helpful in assessing the features of a patient’s disease and the extent of anatomic damage.2. Brower AC. In: Klippel JH, Dieppe PA, eds. Rheumatology. Vol 1. 2nd ed. Philadelphia, Pa: WB Saunders; 1998;5:5.1–5.8. Resnick D et al. In: Kelley WN et al, eds. Textbook of Rheumatology. 5th ed. Philadelphia, Pa: WB Saunders; 1997:626– Resnick D, Yu JS, Sartoris D. Imaging. In: Kelley WN, Harris ED Jr, Ruddy S, et al, eds.Textbook of Rheumatology. 5th ed. Philadelphia, PA: WB Saunders; 1997: Grassi W, De Angelis R, Lamanna G, Cervini C. The clinical features of rheumatoid arthritis. Eur J Radiol. 1998;27(suppl 1):S18-S24.")
9
Radiologisk progression rheumatoid arthritis
100 90 80 70 60 50 40 30 20 10 Erosion score (Larsen and Thoen, 1987) Maximum Score (%) Erosion score (Fuchs et al, 1989) Total score (Larsen and Thoen, 1987) Erosion score (Ferraccioli et al, 1989) Joint-space narrowing score (Ferraccioli et al, 1989) Joint-space narrowing score (Fuchs et al, 1989) Case for early RA treatment—all trials yield similar results. 40%–50% minimum score by 2 to 3 years. By 5 to 6 years, the damage is done. Duration of Rheumatoid Arthritis (Years) Fuchs HA, Pincus T, et al. J Rheumatol 1992;19:1655.
 Maximum Score (%) Erosion score (Fuchs et al, 1989) Total score (Larsen and Thoen, 1987) Erosion score (Ferraccioli et al, 1989) Joint-space narrowing score (Ferraccioli et al, 1989) Joint-space narrowing score (Fuchs et al, 1989) Case for early RA treatment—all trials yield similar results. 40%–50% minimum score by 2 to 3 years. By 5 to 6 years, the damage is done Duration of Rheumatoid Arthritis. (Years) Fuchs HA, Pincus T, et al. J Rheumatol 1992;19:1655.")
10
Change in van der Heijde modified Sharp Score (SHS) of hands from baseline to 10 years according to the level of anti-CCP Syversen, S W et al. Ann Rheum Dis 2008;67: Copyright ©2008 BMJ Publishing Group Ltd.

14
Behandlingsmål ved RA Reducere smerte og inflammation
Forbedre funktionen Reducere/bremse leddestruktion Inducere remission Forbedre overlevelsen During just the last few years, we have learned how to treat RA better, with the patient-oriented goals of relieving symptoms, preventing joint destruction, improving and preserving the quality of life, and, ideally, achieving clinical remission if not actual cure. To this end, the current generation of biologics have been instrumental in reducing pain and inflammation, improving physical function, and retarding and sometimes even halting joint destruction. Thus, these newer DMARDs hold the promise of improving the quality of life and survival. In 2002, we can’t promise much in the way of remissions. Remissions are rare: Spontaneous = rare DMARD-induced = rare Combo DMARD use = induced remissions on few occasions We need surrogate markers for connection between S&S and radiographic destruction. Primer on the Rheumatic Diseases. 12th ed. Atlanta, Ga: The Arthritis Foundation; 2001:

18
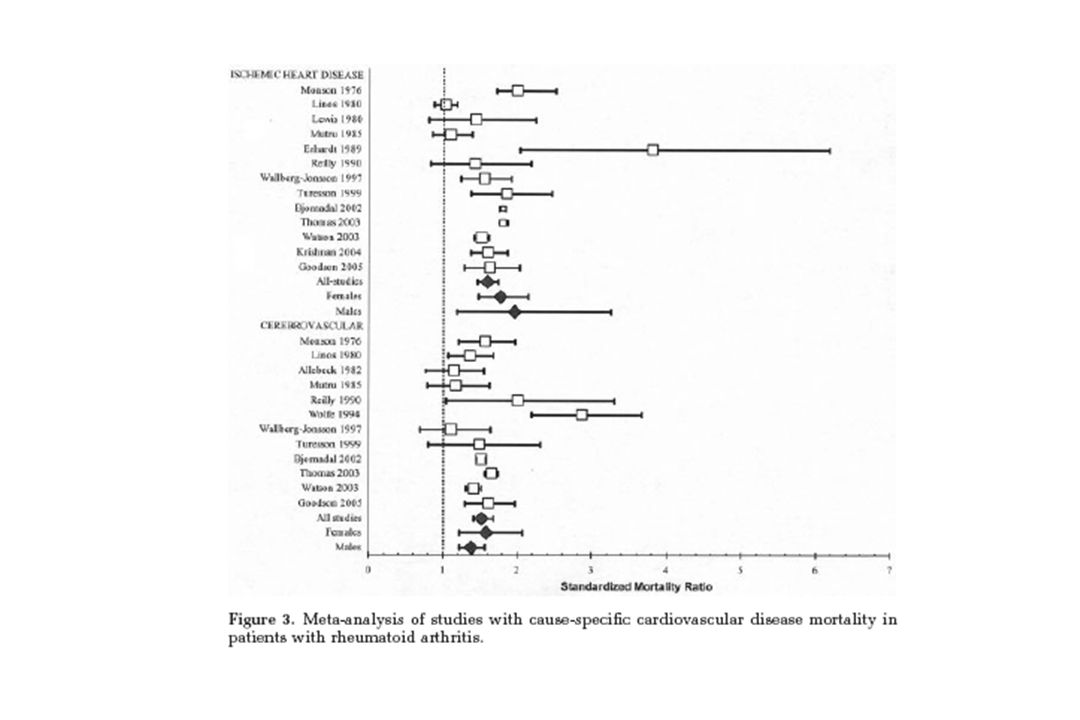
Rekommendation 1 RA er associeret med højere risiko for CV sygdom.
Dette gælder formentligt også AS og PsA Den øgede risiko skyldes både traditionelle risikofaktorer og inflammationen

19
Rekommendation 2 Tilstrækkelig og effektiv sygdomskontrol er nødvendig for at reducere den CV risiko (både TNF-hæmmer og MTX-behandling)
")
20
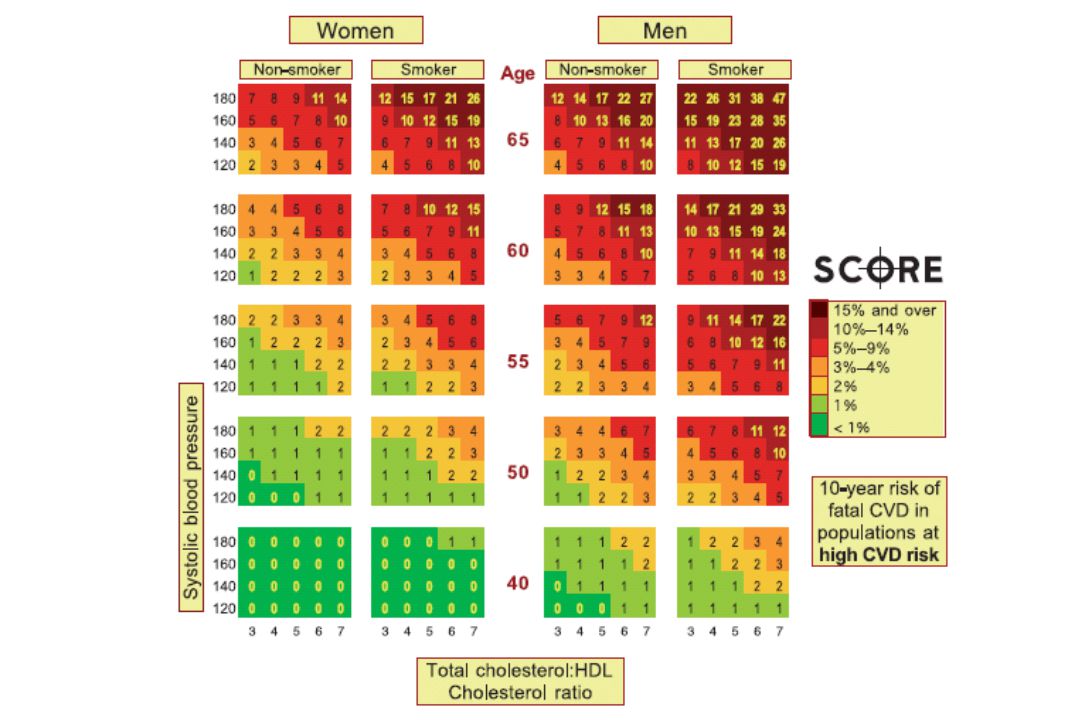
Rekommendation 3 CV risikovurdering ved brug af nationale guidelines anbefales for alle RA-patienter årligt og kan overvejes for AS og PsA Risikovurdering anbefales ved behandlingsskift

22
Rekommendation 4 Risikoscoringsmodel anvendt ved RA skal multipliceres med 1,5 når 2 af 3 kriterier er til stede Sygdomsvarighed mere end 10 år RF eller anti-CCP positiv Tilstedeværelse af visse extraartikulære manifestationer

23
Rekommendation 5 Total cholesterol/HDL cholesterol ratio skal anvendes når SCORE model anvendes

24
Rekommendation 6 Intervention i forhold til nationale retningslinier

25
Rekommendation 7 Statiner, ACE-hæmmere og/eller AT-II-antagonister foretrækkes p.gr.a. deres mulige anti-inflammatoriske effekter

26
Rekommendation 8 Betydningen af COXIBs and de fleste NSAIDs vedrørende CV risiko er ikke endeligt afklaret, men der bør udvises forsigtighed ved brug, især blandt patienter med dokumenteret CV sygdom eller ved tilstedeværelse af risikofaktorer

27
Rekommendation 9 Glukokortikosteroid dosis lavest mulig

28
Rekommendation 10 Anbefal rygestop

Lignende præsentationer