Download præsentationen
Præsentation er lastning. Vent venligst

1
Compliance and Concordance management within Diabetes and Hypertension
Hanne Herborg and Kirsten Pultz Pharmakon Danish College of Pharmacy practice

2
Objectives Participants will in relation to Hypertension and Type 2 Diabetes: Explore the concordance concept and its relation to adherence Acquire knowledge, tools, and skills on how to implement concordance in patient relations in the pharmacy.

3
Background The workshop is based on EuroPharm Forum programmes on diabetes and hypertension The working models are tried out in 2 Danish demonstration projects within these areas: ”Safe and effective use of medicines” The patients are assigned to either a comprehensive or a basic version of the programme. Participants will work with the comprehensive version

4
Structure Presentation of participants and workshop leaders
Integration of concordance and adherence into the EuroPharm Forum model Approach from the Danish demonstration projects Presentation of the service and process in ’Safe and effective use of medicines’ Testing the process Discussion and conclusions

5
Tetsting the process in smaller groups
Assessing the Quick Screening Instrument and medication profile Patient interview Dialoque with the patient tailoring solutions

6
Presentation: Safe and Effective Use of Medicines
Hanne Herborg Director R&D Pharmakon Danish College of Pharmacy Practice Dear Colleagues ¨- Gratefull for chance to present this case- story from DK pharmacy practice -Case about a program, we call SEM - I’ll talk about the practice model, which we have developed

7
Two Danish research programs
“Implementation of drug therapy Improved adherence and self-management among users of anti-hypertensive medicines” Program development From February 2006 to February 2007, the program is being tested in 250 patients in a controlled study comparing a brief and a comprehensive version of the intervention. “Safe and effective use of medicines in Type 2 Diabetes” Programme development Test in 80 patients from October 2006 - We developed it at DCCP as part of a larger research program - the model was tested in 27 patients by 3 pharmacies and 4 GP’s this spring - so it is still very new And it will be tested i a controlled study in the coming year

8
Objectives To develop and evaluate pharmacy based primary care programs aimed at ensuring safe and effective medicine-use among users of Hypertension and Type 2 Diabetes medicines To develop a concordance-partnership between GPs, pharmacy staff, and non-adherent Hypertension and Type 2 Diabetes patients To develop and validate instruments to document the effect of concordance and adherence programs. The objectives of the pilot study are shown on this slide read SLIDE -My plan today is is to give a presentation of how the program was constructed and illustrate how it operates in practice

9
The concordance concept

10
Adherence and concordance - what’s the difference?
Focus on consultation process. Refers to the nature of the relationship A consultation process between a patient and a health care professional in which power is shared and the patients’ perspective is valued Weiss & Britten 2003 Adherence: Focus on patient behaviour Refers to medicine taking as agreed

11
Terminology problems Concordance does not replace adherence
Implementation of drug therapy is still a key issue, and we need terminology for this ‘Informed adherence’ has been suggested as a useful and more precise term than adherence Horne & Weinman 2004 Adherence is not well understood in the Danish context We speak about ‘compliance and concordance management’ We use the term ‘Informed compliance’ to describe medicine taking as agreed

12
Adherence: a complex problem
Our platform is the WHO review 2003: A systems approach is required to understand adherence Not just patient factors as in most compliance research Environment factors Health system factors Treatment, disease Support: network, professionals Patient’s social context and culture Patient factors Aspects: Motivational, emotional, cognitive, behavioural We have chosen the apporach in the WHO review that Ross mentioned yesterday as our primary platform - because of the very strong evidence supporting it To summarise: - Adherence is understood as a complex problem - not just determined by patient factors as most often seen, but a systems approach involving READ SLIDE - and of course also adressing patient factors in the broadest sense - i.e READ SLIDE

13
Program approach Multidimensional program
Systemic and narrative approach to the problem of non-adherence and lack of concordance Clear distinction between intentional and unintentional non-adherence and stages of adherence Pharmaceutical care approach to drug therapy Close partnership with the patient, built up through story-telling and individual coaching With this background (and other models) these are the principles we aimed for - READ SLIDE We wanted it to be a very strong parmacy platform that eventually can lead to several services And/or To one very comprehensive service, comparable to other behaviour change program such as smoking or diet lifestyle change
 these are the principles we aimed for. - READ SLIDE. We wanted it to be a very strong parmacy platform that eventually can lead to several services. And/or. To one very comprehensive service, comparable to other behaviour change program such as smoking or diet lifestyle change.")
14
Program elements Quick screening for non-adherence and identification of problem types Patient story-telling as the key starting point Assessment and possibly adjustment of drug therapy Finding resources in the patient-system Individual coaching, in order to tailor solutions to individual needs and resources Offering relevant reminder technology and/or patient instruction Follow up Close collaboration with patient’s GP So the elements we include now are the following. READ SLIDE - For all these elements we have structured/systematic support

15
Instruments and tools The programs are supported by a considerable number of instruments The core model and instrument is the ’systems-model’ This model supports lateral thinking in the search for causes and resources for problem solution As I said, we have prduced suport for each of the elements: In fact this program is a large toolbox, not a standardised process - So we have a range of instruments, which I will briefly talk about And I will also talk about our main tool , which we call the ’ systems model’ - It is crucial to support lateral thinking in the search for resources

16
The magic bullet? - a dream – not reality
So this is not a simple model Most pharmacies would prefer that we came up with a simple service that would hit the problem rigth on the spot - We did not believe in this magic : One size does not fit all - The evidence speaks against it. --We rather believe that dealing with adherence requires complex professional skills and refined tools used very conciously and not guessing in the dark and throwing your standard solution blind folded

17
Tools for the intervention - 1
Evaluation of medicines and drug related problems Quick Screen Instrument, QSI: Patient experienced problems, lack of concordance/compliance, poor outcome Pharmaceutical care technology: Check for: Interactions, dose regimes and side effects A check of the personal electronic medication profile Indicators for drug related and economic problems The toolbox of the program has the following instruments for the pharmacies and GP’s at this stage: READ SLIDE

18
Tools for the intervention - 2
Counselling and coaching of the patient Interview guide: Motivating interview technique using key words: stage-of change, concordance, self-efficacy Systemic coaching Patient education and information Written, video and Internet based information resources Internet site for patients READ Slide

19
Tools for the intervention - 3
’Reminder’-technologies Technical aids and patient feedback systems Dose dispensing aids SMS-reminders, telephone-reminders Electronic medicine monitor (MEMS) and feedback Blood pressure measurement Patient diaries (paper/internet) Referral tools To GP’s in relation to evaluation of prescriptions To health promotion services: In relation lifestyle related problems, e.g. smoking, overweight and lack of exercise Read SLIIDE GP Referral - is also about diplomatic and appreciative communication -This gives primary care profesionals opportunity to tailor their work
 and feedback. Blood pressure measurement. Patient diaries (paper/internet) Referral tools. To GP’s in relation to evaluation of prescriptions. To health promotion services: In relation lifestyle related problems, e.g. smoking, overweight and lack of exercise. Read SLIIDE. GP Referral - is also about diplomatic and appreciative communication. -This gives primary care profesionals opportunity to tailor their work.")
20
Finding tools that will work - the key to success
The trick however, is not to return to simplistic models, But to have profesional routine to find the right tools, So we need to give the proper support ande training

21
The systems model Medicines Motivation Behaviour Knowledge Lifestyle
Health system Network Health and Symptoms

22
Let’s look at an example
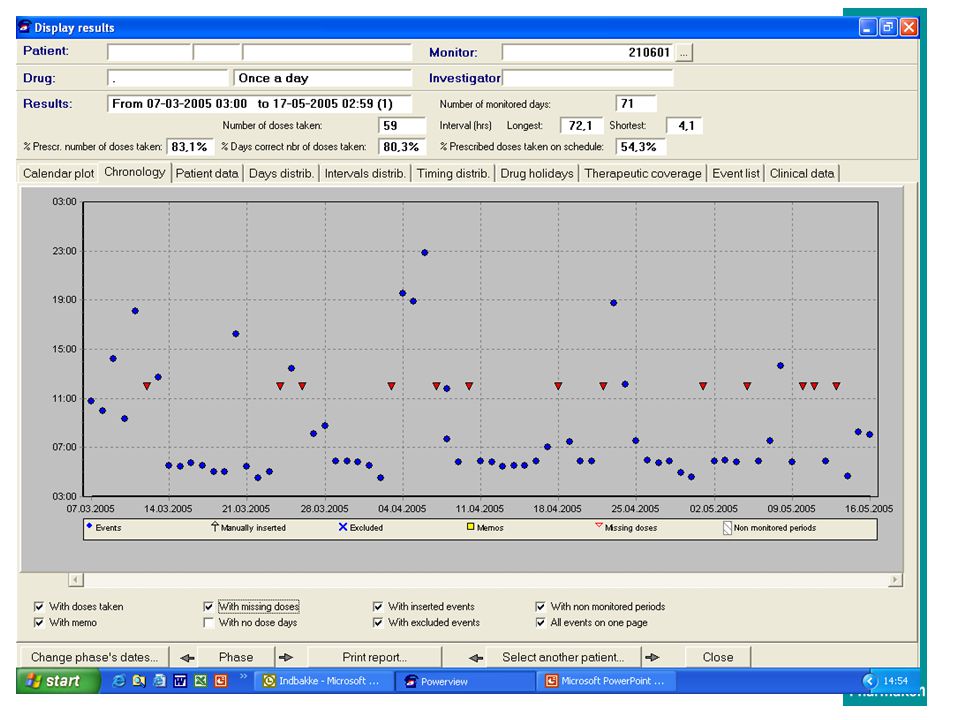
This is a test patient form the Danish Personal Electronic Medication profile (PEM) Let’s say we start with a medication profile looking like this: You notice the drug list and the compliance- graphics the holes indicate a problem of under use in this asthma patient. We all have a profile like this sitting in the DMA. It can be accessed by patients and GP’s and by pharmacise when given a consent by the patient
 Let’s say we start with a medication profile looking like this: You notice the drug list and the compliance- graphics. the holes indicate a problem of under use in this asthma patient. We all have a profile like this sitting in the DMA. It can be accessed by patients and GP’s and by pharmacise when given a consent by the patient.")
23
Story-telling - a method for finding unknown resources
We organise our understanding of the world in stories We often have more than one version of our life-stories Other people have different versions of our stories than our own A story could always have been told otherwise Resources for solutions can perhaps be found in story versions that are less blocked than the patient’s dominating story

24
Jane Lady in her 60’ties, assisting wife, previously health worker
Referred for poor BP control and suspected non-compliance Drugs: Thiazide, beta-blocker Motivated, knows importance of drugs Considers herself adherent Has reminder systems in place Sees no need for interventions Forgets unintentionally when daily routines are broken Believes she can skip a ’few’ times without consequence Knows GP is not happy with BP Does not like MEMS or sms Chooses home-made reminder systems for car and bathroom as solution This patient is not the same, but had a similar profile with her hypertension medcation. We tried to understand her story. READ SLIDE section 1: If you only had this initial talk, you would not see a problem But the PEM gives you more info to explore the stortelling further- - Explaining PEM – of course slips and lapses happen READ Slide section2: -Long talk about how to avoid forgetfullness, when busy. On normal days the blue container by the coffee machine does the job. ’ Ugly blue color on purpose – then you notice´ Not happy with all the smart technology on our list. Likes the home made systems. Time will show if she is persistent

25
Coaching questions -1 Environment reactions
If your doctor were here now, how would he think about your BP and your treatment? Would he be satisfied? What would he think should be done? If I asked your family/network, what would they say? Are they worried about your blood pressure? Do they have wishes or suggestions, that you often hear? How did we get part 2 of the story? This is where the systemic coaching is usefull The shift in positions to other persons is also a shift to other versions of the story. The ’disturb’ the dominating story – I nearly always take my pills OK

26
Coaching questions - 2 Weighing pro’s and con’s
How do the ‘errors’ you do today give you benefits? What are the disadvantages? On a scale from 0-10, how important is the problem of getting your BP down to you? In the best of all worlds… How will the drug treatment of your BP be? In 5 years? In 6 months? What would be the most important change needed to make things go that well? What would be the smallest change needed, to make things move forward? Some of the Q’s are also used im motivational interviewing Like those READ SLIDE

27
Coaching questions - 3 Noticing success Seeing possible goals
Who would notice, if you were taking a drug therapy that you were happy about? How? What would they see you doing? Seeing possible goals From our talk, what would you suggest that we do to get the best possible outcome? Assessment of options What would happen if…… we had your doctor change your medicine? we sent you an sms every day? you had your medicine dose dispensed? I gave you some more information about your illness and your medicine? you came here in the pharmacy to have your BP measured? …..etc. And finally questions to talk about getting to do somthing else… READ SLIDE

28
Finding possible solutions
Container with alarm og feedback(MEMS) Finding possible solutions Referral to GP Dosing aid About Hypertension Medication review About your medication Dose dispensing Patient education Medicines About what you can do Forgetfullness support Behaviour Knowledge Information and counselling SMS Motivation BP measurement at home Diary Brochures Internet Coaching dialogue Individual remembering rules Other Health sites Project homepage Shared apppoinments
 Finding possible solutions. Referral to GP. Dosing aid. About. Hypertension. Medication review. About your. medication. Dose. dispensing. . Patient education. Medicines. About what. you can do. Forgetfullness. support. Behaviour. Knowledge. Information and counselling. SMS. Motivation. BP measurement. at home. Diary. Brochures. Internet. Coaching. dialogue. Individual. remembering. rules. Other. Health sites. Project. homepage. Shared. apppoinments.")
29
Finding possible solutions
Family involvement Coaching in relation to total health situation Involvement of colleagues Lifestyle Health system Network Health and Symptoms Advice on communikation with professionals Referral to GP: symptoms adverse reactions Coaching on transitions e.g. from home to hospital Information on reimbursement and substitution Referral to e.g. smoking cessation Use of Medication Profile

32
Balancing the elements - an exercise requiring knowledge, skills and routine

33
Instructions for the group work
Preparation (10 minutes) - assess the QSI and medication profile using the checklist - identify problems with the blood pressure/diabetes regulation - identify problems with compliance - identify drug related problems Patient interview brief, part I (10 minutes) Problem analysis Identify the most important problems using the visual tool. Find possible solutions (10 minutes) Dialogue with the patient, interview part II: Find resources and tailor solutions (15 minutes)
 - assess the QSI and medication profile using the checklist - identify problems with the blood pressure/diabetes regulation - identify problems with compliance - identify drug related problems. Patient interview brief, part I (10 minutes) Problem analysis. Identify the most important problems using the visual tool. Find possible solutions (10 minutes) Dialogue with the patient, interview part II: Find resources and tailor solutions (15 minutes)")
34
Conclusion Plenary discussion

36
En patienthistorie Karen
Kvinde, 48 år, ryger og kg overvægtig. Har for 4 mdr. siden fået konstateret et ret forhøjet blodtryk Får Thiazider. Lægen har anbefalet vægttab og rygestop. Syntes ikke at BT-behandlingen virker – Har forsat ondt i hovedet. Er ikke kompliant med bt-behandling Ved behandlingens start non-kompliant på grund af glemsomhed Venindes erfaringer har skabt utryghed omkring behandlingen, hvorfor den nu bevidst fravælges. Er ikke motiveret for hverken vægttab, rygestop eller tabletbehandling. Ved kontrol efter 3. Mdrs. behandling er blodtrykket uændret. Nævner ikke overfor lægen, at behandlingen ikke implementeres.

37
Case 1: Henrik, 47 år Inkluderet pga. complianceproblemer (identificeret i Medicinprofilen og Henriks egne udsagn) 1. kontakt QSI viser primært problemer med ubevidst non-compliance Blodtryk måles – er ikke optimalt Henrik vil gerne tage sin medicin Han vil gerne prøve doseringsæske Aftaler, at han sammen med sin kone vil identificere, hvor doseringsæsken skal ligge 2. kontakt: (telefonisk efter 14 dage) Doseringsæsken har hjulpet
 Doseringsæsken har hjulpet.")
38
Case 1: Henrik, 47 år (2) 3. kontakt 4. kontakt
Henrik har fået en ny recept på noget kolesterolsænkende – er lidt frustreret over, at skulle tage mere medicin. Blodtryk: næsten tilfreds Dialog om tankerne om medicinen – og information om det konkrete lægemiddel 4. kontakt Fungerer fortsat med doseringsæske Men han glemmer "natdosis" SMS er en mulighed – han tilmelder sig på projektets hjemmeside

39
Case 1: Henrik, 47 år (3) 5. kontakt: (telefonisk efter 3 uger)
Nu fungerer det – og kolesteroltallet er på vej ned Tilbud om opfølgning

40
Case 2: Karen, 63 år Inkluderet pga. complianceproblemer (identificeret i Medicinprofilen og Karens egne udsagn) og pga. blodtrykkontrol ikke ok QSI viser primært problemer med bevidst non-compliance Blodtryk måles – er ikke optimalt Interview tydeliggør, at Karen har problemer med bivirkninger og hendes holdning er, at medicinen er noget gift Hendes holdning til information er blandet Plan lægges på kort og på længere sigt Karen anbefales at tale med læge om bivirkninger

41
Case 2: Karen, 63 år (2) 2. kontakt: (14 dage senere i skranken)
Karen har talt med lægen og fået recept på en anden medicin. Hun er lidt utryg ved bivirkningerne 3. kontakt: (samtale på apoteket 1 måned efter 1. samtale) Karen er tilfreds med den nye medicin Gener er der, men de er til at leve med Karen tænker stadig over, om fordelene ved medicinen opvejer ulemperne Coaching på motivation Patientuddannelse og skriftligt materiale med hjem
 Karen er tilfreds med den nye medicin. Gener er der, men de er til at leve med. Karen tænker stadig over, om fordelene ved medicinen opvejer ulemperne. Coaching på motivation. Patientuddannelse og skriftligt materiale med hjem.")
42
Case 2: Karen, 63 år (3) 4. kontakt: (samtale på apoteket tre måneder senere) Apoteket har fået tilbagemelding fra læge, om at Karens BT er faldet og den nye medicin ser ud til at fungere – men at hun stadig springer over. De har talt om at Karen selv kan følge sit blodtryk hjemme Samtale med Karen om, hvordan det ser ud nu og opfølgning på spørgsmål fra sidst Karen vil gerne måle blodtryk, køber apparat og får instruktion i brug

Lignende præsentationer












 og skal holdes indenfor de to vandrette grå linjer. Der kan frit vælges farver fra farvepaletterne.>")







