Download præsentationen
Præsentation er lastning. Vent venligst

1
Hvad er spasticitet? Jens Bo Nielsen
Department of Physical Exercise and Sport Science & Department of Neuroscience and Pharmacology Panum Københavns Universitet Jakob Lorentzen Department of Neurorehabilitation, Hvidovre hospital & Department of Neuroscience and Pharmacology Panum

2
Hvorfra stammer begrebet?
Lat. Spasticus; at trække mod sig selv.( 1753 Gout, defined to be a spastic and painful affection ( A spasticity or want of pliancy in the muscular fibres. (

3
Spasticitet – tidlig historie
1841 – Marshall Hall: Decapitated frogs Automatiske bevægelser i ellers paretiske ben – kaldet reflekser (introduceret af Willis). Tonus: Certain degree of firmness. Tonus forårsaget af reflekser 1863 – Sechenev foreslår release of reflex function fra cerebral inhibition 1855 Bentley Todd beskriver early and late rigidity 1880: Brissaud differentierer mellem reflex medieret stivhed og kontrakturer ved hjælp af ischæmi Sherrington beskriver forøgede strækreflekser ved decerebreret rigiditet
. Tonus: Certain degree of firmness. Tonus forårsaget af reflekser – Sechenev foreslår release of reflex function fra cerebral inhibition Bentley Todd beskriver early and late rigidity. 1880: Brissaud differentierer mellem reflex medieret stivhed og kontrakturer ved hjælp af ischæmi Sherrington beskriver forøgede strækreflekser ved decerebreret rigiditet.")
4
Spasticitet – senere historie
Eccles, Lundberg o.a. – introduktion af intracellulær registrering i motorneuroner. Analyse af netværk på dyr. : Farmakologisk behandling af spasticitet introduceres (benzodiazepiner, baklofen o. a.) 1970- : Introduktion af elektrofysiologiske metoder til undersøgelse af patofysiologiske grundlag for spasticitet hos mennesker 1978-: Introduktion af første isokinetiske dynamometre til spasticitetsevaluering 1990erne: Introduktion af Botox
 : Introduktion af elektrofysiologiske metoder til undersøgelse af patofysiologiske grundlag for spasticitet hos mennesker : Introduktion af første isokinetiske dynamometre til spasticitetsevaluering. 1990erne: Introduktion af Botox.")
5
Definition af spasticitet
Spasticity is a motor disorder characterized by a velocity-dependent increase in tonic stretch reflexes (’muscle tone’) with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex, as one component of the upper motor neuron syndrome. Lance, Spasticity: Disordered Motor Control 1980
 with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex, as one component of the upper motor neuron syndrome. Lance, Spasticity: Disordered Motor Control")
6
But in the clinic ”spasticity” is used more broadly:
Increased muscle tone Multiple sclerosis Stroke Spinal cord injury Amyotrophic lateral sclerosis Traumatic brain injury Cerebral palsy Tumors Hereditary spastic paraparesis (Neurolatyrism) (hyperekplexia (startle disease)?) Hyperexcitable tendon jerks (stretch reflexes) Spasms Spastic gait Babinski Increased flexor reflexes and contractures
 (hyperekplexia (startle disease) ) Hyperexcitable tendon jerks. (stretch reflexes) Spasms. Spastic gait. Babinski. Increased flexor reflexes. and contractures.")
8
Den kliniske hverdag SPASM: Definition Forøget muskel tonus Hyperexcitable strækreflekser Forøgede flexor reflexer Spasmer Babinski Kontrakturer? ”disordered sensi-motor control, resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles” Kilde: Pandyan et al. Spasticity , clinical perceptions and neurological realities and meaningful measurements. Disabil Rehabil ;27:2-6.

9
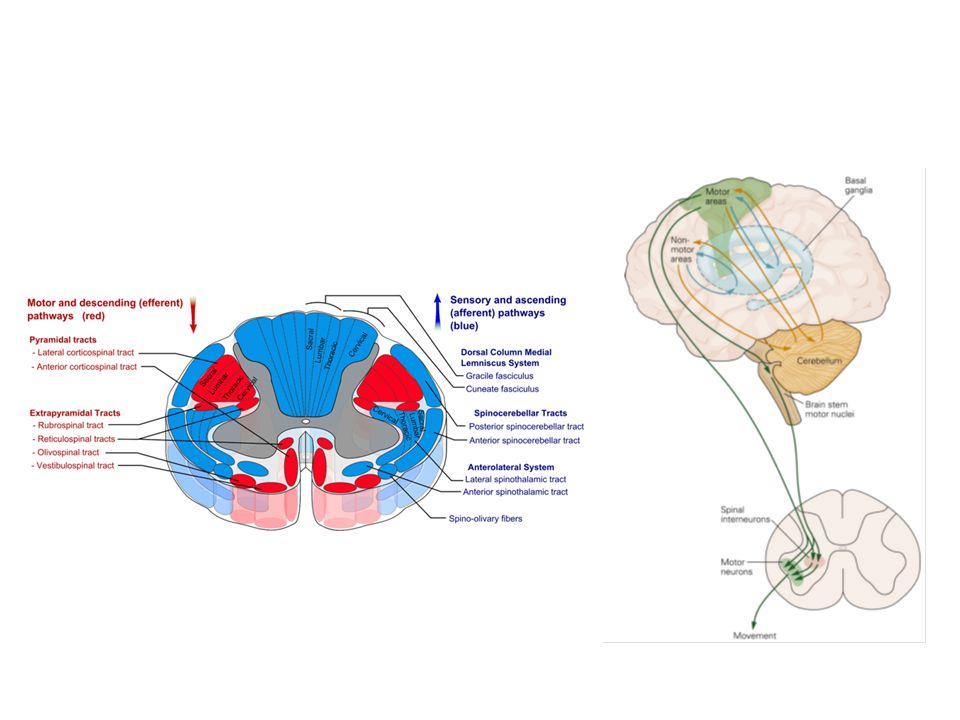
Different pathophysiological mechanisms are involved
Velocity dependent resistance to stretch. Increased stretch reflexes Spasms – sustained activity after input. Role of flexor reflexes, role of Mn properties? Spontaneous muscle activity at ´rest´. = increased muscle tone at rest (and without provocation). Lesion of basal ganglia? Inability to ´relax´ Contractures. Alteration of passive muscle properties Spastic Gait ??
. Lesion of basal ganglia Inability to ´relax´ Contractures. Alteration of passive muscle properties. Spastic Gait")
10
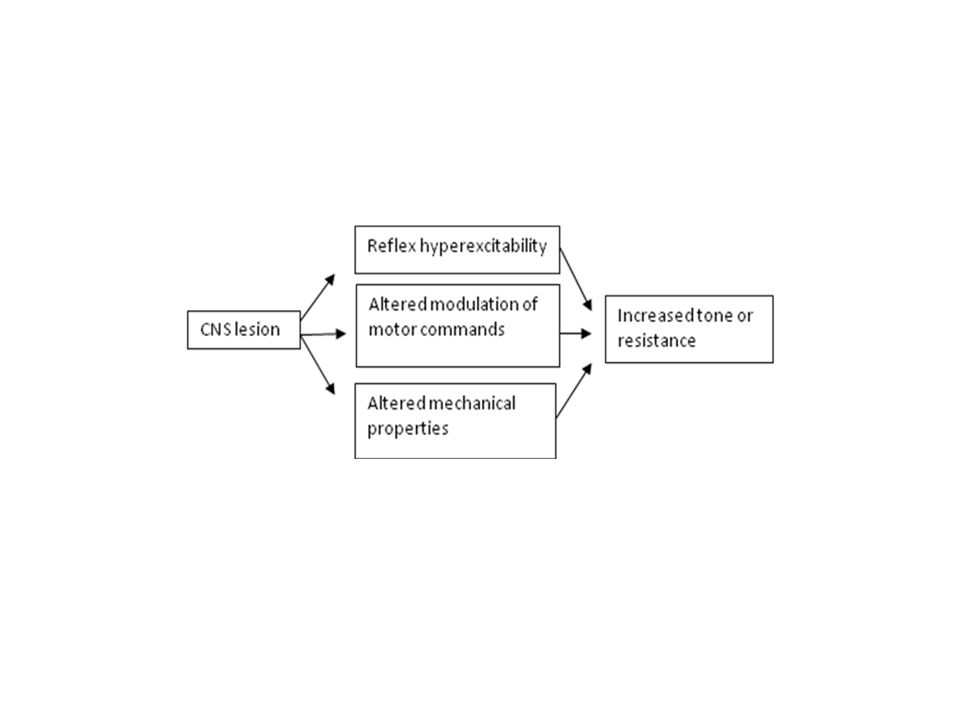
Factors causing hypertonicity
Active stiffness Passive stiffness (Contracture) Afferent (disinhibited spinal reflexes) Efferent (tonic supraspinal drive) Arthrogenetic changes Myogenetic changes Proprioceptive reflexes Cutaneous and nociceptive reflexes (Spastic) dystonia Intra-articular adhesion formation Loss of sacromers in series Spasticity (tonic) Flexor withdrawal reflexes Associated reactions ?synkinesia Adaptive shortening of periarticular connective tissue Increased intra muscular collagen Tendon hyperreflexia and Clonus (phasic) Flexor spasms Cocontraction Reduced lubrication between collagen fibres Disuse atrophy Clasp knife syndrome Clasp knife (with tonic stretch reflex) Increased immature collagen Muscle fibre transformation ST to FT Extensor reflexes Degenerative changes in muscle-tendinous junction Extensor spasms Increased actine-myosin cross-bridge linkage
 Afferent (disinhibited spinal reflexes) Efferent (tonic supraspinal drive) Arthrogenetic changes. Myogenetic changes. Proprioceptive reflexes. Cutaneous and nociceptive reflexes. (Spastic) dystonia. Intra-articular adhesion formation. Loss of sacromers in series. Spasticity (tonic) Flexor withdrawal reflexes. Associated reactions synkinesia. Adaptive shortening of periarticular connective tissue. Increased intra muscular collagen. Tendon hyperreflexia and Clonus (phasic) Flexor spasms. Cocontraction. Reduced lubrication between collagen fibres. Disuse atrophy. Clasp knife syndrome. Clasp knife (with tonic stretch reflex) Increased immature collagen. Muscle fibre transformation ST to FT. Extensor reflexes. Degenerative changes in muscle-tendinous junction. Extensor spasms. Increased actine-myosin cross-bridge linkage.")
11
5 minutters pause til diskussion
Hvilken definition på spasticitet skal vi bruge?

12
Back to basics: Hvad bestemmer muskel ´tonus´?
Passive properties (tendon, connective tissue etc) 2. Active properties (how many cross-bridges?)
 2. Active properties (how many. cross-bridges )")
13
Muskel tonus ”the sensation of resistance felt as one manipulation of a joint through a range of motion, with the subject attempting to relax” Lance and McLoud 1981

15
Hvordan trækker musklen sig sammen? Hvordan forlænger musklen sig?

16
Kontraktur Ref: Singer B et al. Reflex and non-reflex elemanet of
hypertonia in triceps surae muscles following acquired brain injury: implications for rehabilitation. Disabil Rehab, 2001; vol.23 no.17,

17
Ændring i antallet af sacromer
SOL Ref: Shah SB et al. Sacromere number regulation maintained After immobilization in desmin-null mouse skeletal muscle. The Journal of experimental biology 204, (2001).
.")
18
Behandling Evidens for øget ROM Ingen ændring i spasticitet
Ikke øget funktionsniveau Ref: Mortenson PA, Janice JE. The use of casts in the management of joint mobility And hypertonia following brain injury in Adults: a systematic review. Physical Therapy Vol 83 number 7, July 2003.

19
Behandling - udspænding
Ikke evidens for effekt. ”Four weeks of daily stretch has little or no effect on wrist contracture after stroke: a randomised controlled trial Ref: Horsley SA et al. Four weeks of dayily stretch has little or no effect on wrist contracture after stroke: a randomised controlled trial Australian Journal of physiotherapy 53: Anbefaling – langvarigt stræk > 20 min – 12 timer pr dag Ref: Harvey LA, Herbert RD. Muscle stretching for treatment and prevention of contracture in people with spinal cord injury. Spinal Cord. 2002 Jan; 40(1):1-9.
:1-9.")
20
Elektromekanisk kobling

21
Cross-bridge formation

22
Hvis der ikke findes aktivitet i nerverne (ingen AP) er der heller ikke ret meget Ca i muskelcellerne og derfor ingen dannelse af krydsbroer – dødsstivhed bidrager med andre ord ikke til musklernes stivhed (tonus) i hvile – dvs udelukkende bindevæv o.a. bestemmer stivheden i hvile

23
NB: Motorneuronerne er pr definition langt fra deres fyringstærskel i hvilesituationen – og sender således ingen aktionspotentialer til musklerne. Men er vi i den kliniske situation altid sikre på at patienten er i hvile? Findes der forskellige grader af hvile? Hvad har betydning for det?

24
Hvad bestemmer aktiviteten i motorneuroner? Den forenklede model.
Descenderende supraspinalt input Mn egenskaber Mn er ikke aktive spontant! (men: kramper + spasmer?) Sensorisk input
 Sensorisk input.")
25
Hvad bestemmer aktiviteten i motorneuroner?

26
Budskabet er at der ikke er øget tonus i musklerne medmindre der er forandringer i musklernes bindebæv olign (kontrakturer og forstadier) eller aktivitet i motorneuronerne. Aktiviteten i motorneuronerne kan være ´spontan´ - slapper patienten af? – er der tale om dystoni? – eller provokeret af voluntær aktivitet eller sensorisk input (spasticitet) Klassifikation: Passiv Aktiv Reflex medieret Supraspinalt medieret Slapper patient af? Patologisk årsag – fx affektion af basal kerner

27
Behandling afhænger af symptom
Spasticitet: Behandling nødvendig/hensigtsmæssig.? Fysioterapi, træning, antispastisk medicinering (ikke botox!) Dystoni: Muligvis Botox, men langsigtet virkning ikke klart dokumenteret Kontrakturer: Udstrækning , gipsning, men dokumentation for langsigtet effekt mangler Spasmer: Behandling nødvendig/Hensigtsmæssig? Antispastisk medicinering
 Dystoni: Muligvis Botox, men langsigtet virkning ikke klart dokumenteret. Kontrakturer: Udstrækning , gipsning, men dokumentation for langsigtet effekt mangler. Spasmer: Behandling nødvendig/Hensigtsmæssig Antispastisk medicinering.")
28
Hvad er årsagen til spastictet?

29
Dystoni Parese Ataxi Spasticitet

30
Årsager til spasticitet i DK
Apopleksi ( pr år – stigende – 50 % varigt mén) – heraf ca % spasticitet Hjernetraumer ( pr år) – heraf % spasticitet MS ( pr år) – heraf % spasticitet Rygmarvslæsion ( pr år) – heraf % spasticitet Cerebral parese o.lign. (125 pr år) - ?
 – heraf ca % spasticitet. Hjernetraumer ( pr år) – heraf % spasticitet. MS ( pr år) – heraf % spasticitet. Rygmarvslæsion ( pr år) – heraf % spasticitet. Cerebral parese o.lign. (125 pr år) -")
31
Spasticitet skyldes ikke læsion af pyramidebanen
Evidence from monkeys NO: Towers 1940 NO: Lawrence & Kuypers. The functional organization of the motor system in the monkey. I. The effects of bilateral pyramidal lesions. Brain Mar;91(1):1-14. Evidence from human NO: Sherman et al. J Neurol Sci Apr 15;175(2): NO: Nathan PW Effects on movement of surgical incisions into the human spinal cord. Brain Apr;117 ( Pt 2): Yes: Paulson et al. Arch Neurol Jan;43(1):93-5.
:1-14. Evidence from human. NO: Sherman et al. J Neurol Sci Apr 15;175(2): NO: Nathan PW Effects on movement of surgical incisions into the human spinal cord. Brain Apr;117 ( Pt 2): Yes: Paulson et al. Arch Neurol Jan;43(1):93-5.")
32
Hjernelæsion involverer almindeligvis mange strukturer

33
Pathophysiological mechanisms in spasticity
Gr. II pathways Postactivation depression

34
Control of reciprocal inhibition in healthy human subjects

35
Reciprocal inhibition in patients with spasticity
Crone C, Nielsen J, Petersen N, Ballegaard M & Hultborn H. (1994). Brain 117, Crone C, Johnsen LL & Nielsen J (2000). Clinical neurophysiology suppl 53, Morita H, Crone C, Christenhuis D, Petersen NT & Nielsen JB. (2001). Brain. 124(Pt 4), Crone C, Johnsen LL, Biering-Sørensen F & Nielsen JB (2003). Appearance of reciprocal facilitation in patients with spasticity. Brain, 126(Pt 2):
. Brain 117, Crone C, Johnsen LL & Nielsen J (2000). Clinical neurophysiology suppl 53, Morita H, Crone C, Christenhuis D, Petersen NT & Nielsen JB. (2001). Brain. 124(Pt 4), Crone C, Johnsen LL, Biering-Sørensen F & Nielsen JB (2003). Appearance of reciprocal facilitation in patients with spasticity. Brain, 126(Pt 2):")
36
Reciprocal inhibition in stroke patient
Before stroke After stroke

37
Reciprocal inhibition is impaired in the legs but not the arms in ADPSP subjects

38
In spastic patients reciprocal inhibition cannot be appropriately modulated during extension-flexion movements Patients Healthy subjects Healthy subjects without reciprocal inhibition Morita H, Crone C, Christenhuis D, Petersen NT, Nielsen JB Modulation of presynaptic inhibition and disynaptic reciprocal Ia inhibition during voluntary movement in spasticity. Brain 2001;124:826-37

39
Turning off plateau potentials by reciprocal inhibition
Turning off plateau potentials by reciprocal inhibition. Towards a functional understanding of spasticity? Hounsgaard J, Hultborn H,Jespersen B, Kiehn O. J. Physiol. 1988; 405:

Lignende præsentationer


















 Rød løber Tid: 30 minutter. Spilleregler for dagen.>")
