Download præsentationen
Præsentation er lastning. Vent venligst

1
Ledende overlæge, dr. med. Medicinsk Afdeling, Hospitalsenheden Vest
953,1,2,1,0,1,1,1,1,1,1,1,1,0 Item 1 Item 2 Item 3 Item 4 Item 5 Item 6 Item 7 Item 8 Item 9 0,0,0,0,0,0,0,0,0,0 AK-behandling – de mange regimer Steen Husted Ledende overlæge, dr. med. Medicinsk Afdeling, Hospitalsenheden Vest 2014

2
Virchow’s Triade og trombedannelse
Venøs stase Hyperkoagulabel tilstand Karskade Beskrevet af Rudolf Virchow for 150 år siden Heraf fremgår, at forandring i blodflow, karskade og aktivering af koagulationen kan føre til trombedannelse The German Pathologist Rudolf Virchow is attributed with developing the concept of hypercoagulability over 160 years ago. He postulated that there were 3 conditions necessary to lead to thrombosis: changes in the vessel wall (vascular injury, leading to exposure of the highly thrombogenic subendothelial matrix), alterations in blood flow (stasis), and activation of coagulation factors within the blood (later termed hypercoagulability). This concept—called Virchow’s triad—remains central to the modern understanding of thrombogenesis. Reference Joist JH. Hypercoagulability: introduction and perspective. Semin Thromb Hemost. 1990;16: Joist JH. Semin Thromb Hemost. 1990;16:
, alterations in blood flow (stasis), and activation of coagulation factors within the blood (later termed hypercoagulability). This concept—called Virchow’s triad—remains central to the modern understanding of thrombogenesis. Reference. Joist JH. Hypercoagulability: introduction and perspective. Semin Thromb Hemost. 1990;16: Joist JH. Semin Thromb Hemost. 1990;16:")
3
VTE: A strong relationship between DVT and PE
About 50% of patients with proximal DVT of the leg have asymptomatic PE1 Migration Embolus DVT (mainly asymptomatic) is found in around 80% of patients with PE2 Thrombus 1. Pesavento R, et al. Minerva Cardioangiol 1997;45:369–375 2. Girard P, et al. Chest 1999;116:903–908 3
 is found in around 80% of patients with PE2. Thrombus. 1. Pesavento R, et al. Minerva Cardioangiol 1997;45:369– Girard P, et al. Chest 1999;116:903–")
4
Kronisk atrieflimren og muraltrombe

5
En udviklingsproces af aterosklerose
Aterotrombose En udviklingsproces af aterosklerose Normal “Fatty Streak” Fibrøst plaque Aterosklerotisk plaque Plaqueruptur Trombose AMI Iskæmisk apopleksi Bentab Blodstrøm normal Blodstrøm nedsat Blodstrøm kollateral Ingen symtomer Symptomer ved belastning. Angina, TCI, Claudicatio Symptomer i hvile Nekrose Kardiovaskulær død Stigende alder

6
Nogle antitrombotiske præparater
Angrebspunkt Mekanisme Præparat Trombocyt COX-1 hæmning ASA ADP-receptor blokering Clopidogrel, prasugrel, ticagrelor GPIIb/IIIa receptor blokering Abciximab m.fl. Vit. K-afhængige Hæmning af -carboxylering Warfarin koag. proteiner Phenprocoumon Serin proteaser Potensering af AT UFH LMWH Pentasaccharider Trombin Direkte blokering af aktivt site Hirudin m.fl. Dabigatran etexilat Faktor Xa Direkte blokering af aktivt site Rivaroxiban Apixaban

7
Targets for long-term antithrombotic treatment
Tissue factor Plasma clotting cascade * Prothrombin * Thrombin * Fibrinogen Fibrin Thrombus Platelet aggregation Conformational activation of GPIIb/IIIa Collagen Thrombin Tx A2 ADP AT Aspirin Clopidogrel Prasugrel Ticagrelor GPIIb/IIIa inhibitors Dabigatran etexilate Factor Xa * Fondaparinux Idraparinux LMWH Rivaroxaban Apixaban Edoxaban Betrixaban PAR1 PAR1-inhib Warfarin*

8
Perorale vitamin K-antagonister
Warfarin Phenprocoumon (Marevan) (Marcoumar) Absorption Næsten komplet Næsten komplet Proteinbinding 99% 99% Max. effekt timer 8-72 timer Metabolisering Lever Lever T½ plasma timer timer Ophør efter stop 3-5 døgn 7-14 døgn Ny steady-state ca. 7 døgn ca. 28 døgn
 (Marcoumar) Absorption Næsten komplet Næsten komplet. Proteinbinding 99% 99% Max. effekt timer 8-72 timer. Metabolisering Lever Lever. T½ plasma timer timer. Ophør efter stop 3-5 døgn 7-14 døgn. Ny steady-state ca. 7 døgn ca. 28 døgn.")
9
INR: En markør for komplikationer
INR interval Incidens pr. 100 behandlingsår < 2 2 - 3 3 - 4 4 - 5 > 5 2 4 6 8 10 ASPECT study Tromboemboli Blødning

10
Effektiv, men vanskelig
AK-behandling Effektiv, men vanskelig Risiko for blødning tiltager med 40% for hvert INR-point over 4 INR. Risiko for trombose tiltager ved INR < 1,5. Snævert terapeutisk interval. Stor variation i vedligeholdelsesdosis. Betydelig biologisk variation (0,7 INR ved 2-4 INR under steady-state). Problemer med tolkning af INR-svar i forhold til dosisændringer. Talrige lægemiddelinteraktioner Interaktion med kost
. Problemer med tolkning af INR-svar i forhold til dosisændringer. Talrige lægemiddelinteraktioner. Interaktion med kost.")
11
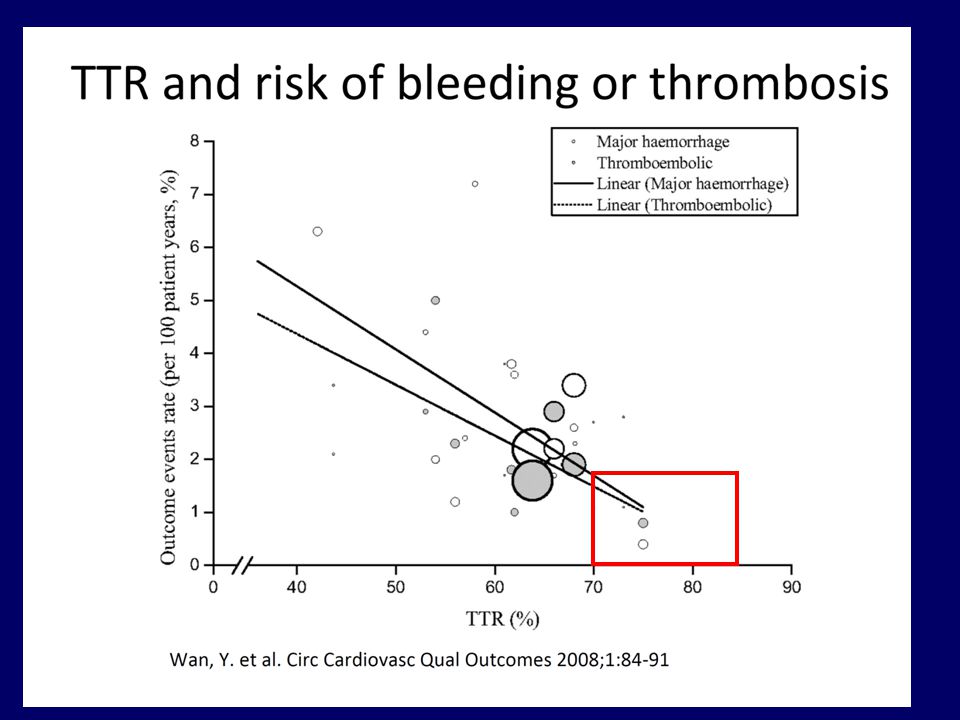
Kvalitet af VKA-behandling

12
Kvalitet af VKA behandling
TTI Tid i terapeutisk interval TTR Time in Therapeutic Range

16
Hovedresultater Pooled Estimate (RR) Self Testing 0.5 0.47 0.56 (NS)
Self Management Self Testing Thromboembolic events 0.5 0.47 0.56 (NS) All-cause mortality 0.64 0.55 1.12 (NS)
 All-cause mortality (NS)")
17
Indikationer for non-VKA orale antikoagulantia (NOAKs)
Ortopædkirurgi venøs tromboseprofylakse Apixaban, rivaroxaban og dabigatran etexilat Atrieflimren – kardioemboli profylakse Apixaban 5 mg BID Rivaroxaban 20 mg OD Dabigatran etexilat 110 eller 150 mg BID Venøs tromboemboli – akut behandling og sekundær profylakse Rivaroxaban 15 mg BID 3 uger fulgt af 20 mg OD Apixaban 10 mg BID 1 uge fulgt af 5 mg BID Apixaban sekundær profylakse 2.5 mg BID Dabigatran etexilate 150 mg BID (+initial bridging med LMWH) Akutte koronare syndromer – sekundær profylakse Rivaroxaban 2.5 mg BID
 Akutte koronare syndromer – sekundær profylakse. Rivaroxaban 2.5 mg BID.")
18
Venous thromboembolism Clinical presentation
DVT PE PFS

19
Phase III VTE treatment study designs
Trial name Design Initial treatment with LMWH/ fondaparinux Treatment duration (months) Long-term treatment regimen Active comparator Principal safety endpoint EINSTEIN DVT (rivaroxaban) OL No 3, 6 or 12 Once daily LMWH/VKA Major plus CRNM bleeding EINSTEIN PE EINSTEIN EXT DB 6 or 12 Placebo Major bleeding RE-COVER (dabigatran) Yes* 6 Twice daily Warfarin Bleeding events RE-COVER II Yes RE-MEDY 18 RE-SONATE AMPLIFY (apixaban) LMWH/ Warfarin Bleeding AMPLIFY-EXT 12 HOKUSAI (edoxaban) Once daily† Heparin/ Warfarin Major or CRNM bleeding References EINSTEIN DVT & EXT Studies. EINSTEIN Investigators. N Engl J Med 2010 (TBC) EINSTEIN PE Study. Trial ID: NCT RE-COVER Study. Schulman et al. N Engl J Med 2009;361:2342–2352 RE-COVER II. Trial ID: NCT RE-MEDY Study. Trial ID: NCT RE-SONATE Study. Trial ID: NCT AMPLIFY Study. Trial ID: NCT AMPLIFY-EXT Study. Trial ID: NCT Hokusai Study. Trial ID: NCT All trial information available at: Accessed 12 November 2010 *Median=9 days; †Two 30 mg tablets. CRNM, clinically relevant non-major bleeding 19 19 19
 Long-term treatment regimen. Active comparator. Principal safety endpoint. EINSTEIN DVT (rivaroxaban) OL. No. 3, 6 or 12. Once daily. LMWH/VKA. Major plus CRNM bleeding. EINSTEIN PE. EINSTEIN EXT. DB. 6 or 12. Placebo. Major bleeding. RE-COVER (dabigatran) Yes* 6. Twice daily. Warfarin. Bleeding events. RE-COVER II. Yes. RE-MEDY. 18. RE-SONATE. AMPLIFY (apixaban) LMWH/ Warfarin. Bleeding. AMPLIFY-EXT. 12. HOKUSAI (edoxaban) Once daily† Heparin/ Warfarin. Major or CRNM bleeding. References. EINSTEIN DVT & EXT Studies. EINSTEIN Investigators. N Engl J Med 2010 (TBC) EINSTEIN PE Study. Trial ID: NCT RE-COVER Study. Schulman et al. N Engl J Med 2009;361:2342–2352. RE-COVER II. Trial ID: NCT RE-MEDY Study. Trial ID: NCT RE-SONATE Study. Trial ID: NCT AMPLIFY Study. Trial ID: NCT AMPLIFY-EXT Study. Trial ID: NCT Hokusai Study. Trial ID: NCT All trial information available at: Accessed 12 November *Median=9 days; †Two 30 mg tablets. CRNM, clinically relevant non-major bleeding")
20
Major bleeding in randomised trials of NOAC- versus VKA for VTE
p Dabigatran RE-COVER 1.6% 1.9% n.s. RE-COVER-II 1.2% 1.7% RE-MEDY 0.9% 1.8% Rivaroxaban EINSTEIN DVT 0.8% EINSTEIN PE 1.1% 2.2% p=0.0032 Apixaban AMPLIFY 0.6% p <0.001

21
EINSTEIN DVT and EINSTEIN PE studies
Rivaroxaban clinical development EINSTEIN DVT and EINSTEIN PE studies Randomized, open-label, event-driven, non-inferiority studies of identical design with a priori specified combined analyses 15 mg bid Confirmed DVT without symptomatic PE1 N=3449 N=8282 Rivaroxaban Day 1 Day 21 Enoxaparin bid for at least 5 days + VKA, INR 2.0–3.0 Confirmed PE with or without symptomatic DVT2 N=4833 Predefined treatment period of 3, 6, or 12 months 20 mg od 30-day post-study treatment period R EINSTEIN DVT and EINSTEIN PE: study design Rivaroxaban doses of 15 mg bid for the initial treatment of VTE and 20 mg od for long-term secondary prevention were investigated in the phase III EINSTEIN DVT and EINSTEIN PE studies A compression ultrasound was used to confirm DVT in the DVT study, and a perfusion lung scan (PLS) was used to confirm PE in the PE study Patients were randomized to receive open-label oral rivaroxaban 15 mg od or conventional therapy (pre-randomization treatment was permitted for up to 48 hours) From day 21, patients were administered open-label rivaroxaban 20 mg od for a predefined treatment period of up to a total of 3, 6 or 12 months At 3 weeks, a repeat PLS was performed in the initial 400 patients in the PE study to confirm the dose of rivaroxaban (this objective test is needed to compare with baseline and permit the efficacy assessment). In the other treatment arm, an open-label low-molecular-weight heparin was administered bid for at least 5 days, until patients meet a target INR of 2–3 Additionally, an open-label dose-adjusted vitamin K antagonist (VKA; acenocoumarol or warfarin), with an international normalized ratio (INR) target of 2–3, was administered for the duration of the study Patients were followed-up during a 30-day observation period More details An open-label study design was employed for EINSTEIN DVT and PE to ensure that the findings reflect the current standard of care in clinical practice, and several measures have been implemented to reduce the potential for bias Rivaroxaban treatment is initiated at 15 mg bid in the VTE treatment programme to provide greater thrombus reduction during the first 3 weeks following VTE, when the risk of recurrence/further thromboembolic events is at its highest. Subsequently, the once-daily 20 mg dose is given for chronic, longer-term use Abbreviations bid, twice daily; DVT, deep vein thrombosis; INR, international normalized ratio; od, once daily; PE, pulmonary embolism; VKA, vitamin K antagonist References The EINSTEIN Investigators. N Engl J Med 2010;363:2499–510 The EINSTEIN–PE Investigators. N Engl J Med 2012;366:1287–97 Primary efficacy outcome: first recurrent VTE Principal safety outcome: first major or non-major clinically relevant bleeding 1. The EINSTEIN Investigators. N Engl J Med The EINSTEIN–PE Investigators. N Engl J Med 2012 21
 was used to confirm PE in the PE study. Patients were randomized to receive open-label oral rivaroxaban 15 mg od or conventional therapy (pre-randomization treatment was permitted for up to 48 hours) From day 21, patients were administered open-label rivaroxaban 20 mg od for a predefined treatment period of up to a total of 3, 6 or 12 months. At 3 weeks, a repeat PLS was performed in the initial 400 patients in the PE study to confirm the dose of rivaroxaban (this objective test is needed to compare with baseline and permit the efficacy assessment). In the other treatment arm, an open-label low-molecular-weight heparin was administered bid for at least 5 days, until patients meet a target INR of 2–3. Additionally, an open-label dose-adjusted vitamin K antagonist (VKA; acenocoumarol or warfarin), with an international normalized ratio (INR) target of 2–3, was administered for the duration of the study. Patients were followed-up during a 30-day observation period. More details. An open-label study design was employed for EINSTEIN DVT and PE to ensure that the findings reflect the current standard of care in clinical practice, and several measures have been implemented to reduce the potential for bias. Rivaroxaban treatment is initiated at 15 mg bid in the VTE treatment programme to provide greater thrombus reduction during the first 3 weeks following VTE, when the risk of recurrence/further thromboembolic events is at its highest. Subsequently, the once-daily 20 mg dose is given for chronic, longer-term use. Abbreviations. bid, twice daily; DVT, deep vein thrombosis; INR, international normalized ratio; od, once daily; PE, pulmonary embolism; VKA, vitamin K antagonist. References. The EINSTEIN Investigators. N Engl J Med 2010;363:2499–510. The EINSTEIN–PE Investigators. N Engl J Med 2012;366:1287–97. Primary efficacy outcome: first recurrent VTE. Principal safety outcome: first major or non-major clinically relevant bleeding. 1. The EINSTEIN Investigators. N Engl J Med The EINSTEIN–PE Investigators. N Engl J Med")
22
EINSTEIN DVT and EINSTEIN PE pooled analysis: primary efficacy outcome
Methods of VTE treatment EINSTEIN DVT and EINSTEIN PE pooled analysis: primary efficacy outcome 0.5 3.0 2.5 2.0 1.5 1.0 0.0 Rivaroxaban N=4150 Enoxaparin/VKA N=4131 30 60 90 120 150 180 210 240 270 300 330 360 Time to event (days) Cumulative event rate (%) HR=0.89; p non-inferiority <0.0001 Mean time in therapeutic range = 61.7% EINSTEIN DVT and EINSTEIN PE pooled analysis: primary efficacy outcome Among patients with acute symptomatic DVT without PE or PE with or without DVT treated for 3, 6 or 12 months, the single-drug approach with oral rivaroxaban showed non-inferiority for the primary efficacy outcome of symptomatic recurrent VTE, compared with the current standard therapy (86 events [2.1%] vs 95 events [2.3%], respectively; HR=0.89; 95% CI 0.66–1.19; p< for non-inferiority). Reference Buller HR, for the EINSTEIN Investigators. American Society of Hematology 54th Annual Meeting and Exposition. Atlanta, GA, USA, 8–11 December 2012 Number of patients at risk Rivaroxaban 4150 4018 3969 3924 3604 3579 3283 1237 1163 1148 1102 1034 938 Enoxaparin/VKA 4131 3932 3876 3826 3523 3504 3236 1215 1149 1109 1071 1019 939 ITT population Buller HR, for the EINSTEIN Investigators. ASH, December 2012 22
 Cumulative event rate (%) HR=0.89; p non-inferiority < Mean time in therapeutic range = 61.7% EINSTEIN DVT and EINSTEIN PE pooled analysis: primary efficacy outcome. Among patients with acute symptomatic DVT without PE or PE with or without DVT treated for 3, 6 or 12 months, the single-drug approach with oral rivaroxaban showed non-inferiority for the primary efficacy outcome of symptomatic recurrent VTE, compared with the current standard therapy (86 events [2.1%] vs 95 events [2.3%], respectively; HR=0.89; 95% CI 0.66–1.19; p< for non-inferiority). Reference. Buller HR, for the EINSTEIN Investigators. American Society of Hematology 54th Annual Meeting and Exposition. Atlanta, GA, USA, 8–11 December Number of patients at risk. Rivaroxaban Enoxaparin/VKA ITT population. Buller HR, for the EINSTEIN Investigators. ASH, December")
23
EINSTEIN DVT and EINSTEIN PE pooled analysis: principal safety outcome
Methods of VTE treatment EINSTEIN DVT and EINSTEIN PE pooled analysis: principal safety outcome First major or clinically relevant non-major bleeding Cumulative event rate (%) Rivaroxaban N=4130 Enoxaparin/VKA N=4116 30 60 90 120 150 180 210 240 270 300 330 360 14 10 12 8 6 4 2 Time to event (days) Rivaroxaban n/N (%) Enoxaparin/VKA n/N (%) HR (95% CI) p-value 388/4130 (9.4) 412/4116 (10.0) 0.93 (0.81–1.06) p=0.27 EINSTEIN DVT and EINSTEIN PE pooled analysis: principal safety outcome The rates of the principal safety outcome (defined as the composite of major bleeding and non-major clinically relevant bleeding) were similar (388 events [9.4%] vs 412 events [10.0%] for rivaroxaban and standard therapy, respectively; HR=0.93; 95% CI 0.81–1.06; p=0.272 ). Reference Buller HR, for the EINSTEIN Investigators. American Society of Hematology 54th Annual Meeting and Exposition. Atlanta, GA, USA, 8–11 December 2012 Number of patients at risk Rivaroxaban 4130 3768 3671 3406 3270 3210 1928 1051 1009 936 878 853 453 Enoxaparin/VKA 4116 3738 3618 3330 3186 3125 1711 1025 981 907 857 823 369 Safety population Buller HR, for the EINSTEIN Investigators. ASH, December 2012 23
 Rivaroxaban. N=4130. Enoxaparin/VKA. N= Time to event (days) Rivaroxaban n/N (%) Enoxaparin/VKA n/N (%) HR (95% CI) p-value. 388/4130 (9.4) 412/4116 (10.0) 0.93 (0.81–1.06) p=0.27. EINSTEIN DVT and EINSTEIN PE pooled analysis: principal safety outcome. The rates of the principal safety outcome (defined as the composite of major bleeding and non-major clinically relevant bleeding) were similar (388 events [9.4%] vs 412 events [10.0%] for rivaroxaban and standard therapy, respectively; HR=0.93; 95% CI 0.81–1.06; p=0.272 ). Reference. Buller HR, for the EINSTEIN Investigators. American Society of Hematology 54th Annual Meeting and Exposition. Atlanta, GA, USA, 8–11 December Number of patients at risk. Rivaroxaban Enoxaparin/VKA Safety population. Buller HR, for the EINSTEIN Investigators. ASH, December")
24
DVT (minus cancer) – initial behandling 1
DVT (minus cancer) – initial behandling 1. linie: Alle patienter én af nedenstående behandlinger VKA + vægtbaseret LMH NOAK Intravenøs UFH styret med APTT måling kan anvendes i stedet for LMH hos indlagte patienter i tilfælde af nyreinsufficiens, svær adipositas, høj blødningsrisiko Katetervejledt lokal administreret trombolyse plus intravenøs UFH hos særlige patienter efter rådgivning fra trombosecenter 2. linie: NOAK Lægemiddelvalg træffes af læge og patient i fællesskab efter samlet individuel vurdering, på baggrund af effekt og bivirkninger, medikamentspecifikke interaktionspotentialer, patientønske og –compliance 2. linie: VKA + vægtbaseret LMH
 – initial behandling 1. linie: Alle patienter én af nedenstående behandlinger. VKA + vægtbaseret LMH. NOAK. Intravenøs UFH styret med APTT måling kan anvendes i stedet for LMH hos indlagte patienter i tilfælde af nyreinsufficiens, svær adipositas, høj blødningsrisiko Katetervejledt lokal administreret trombolyse plus intravenøs UFH hos særlige patienter efter rådgivning fra trombosecenter 2. linie: NOAK Lægemiddelvalg træffes af læge og patient i fællesskab efter samlet individuel vurdering, på baggrund af effekt og bivirkninger, medikamentspecifikke interaktionspotentialer, patientønske og –compliance 2. linie: VKA + vægtbaseret LMH")
25
DVT (cancer) – initial behandling Alle patienter én af nedenstående behandlinger
1. linie: vægtbaseret dalteparin eller tinzaparin 2. linie: NOAK Intravenøs UFH styret med APTT måling kan anvendes i stedet for LMH hos indlagte patienter i tilfælde af nyreinsufficiens, svær adipositas, høj blødningsrisiko Katetervejledt lokal administreret trombolyse plus intravenøs UFH hos særlige patienter efter rådgivning fra trombosecenter Ved kontraindikation for heparinbehandling

26
LE (minus cancer) – initial behandling Alle patienter én af nedenstående behandlinger
1. linie: VKA + vægtbaseret LMH eller NOAK 1. linie: Trombolyse + UFH + VKA Til lavrisiko patienter uden kredsløbspåvirkning og patienter uden betydende påvirkning af højre ventrikel UFH i stedet for LMH hos indlagte patienter i tilfælde af nyreinsufficiens, svær adipositas, høj blødningsrisiko 2. linie: NOAK/vægtbaseret LMH+VKA Til højrisiko patienter vurderet ud fra kredsløbspåvirkning og påvirkning af højre ventrikel 2. line: Højrisiko patienter med kontraindikation for trombolyse konfereres med thoraxkirurger m.h.p. embolektomi

27
LE (cancer) – initial behandling Alle patienter én af nedenstående behandlinger
1. linie: Vægtbaseret dalteparin 1. linie. Trombolyse + UFH/dalteparin Til lavrisiko patienter uden kredsløbspåvirkning og patienter uden betydende påvirkning af højre ventrikel 2. linie: Fondaparinux eller NOAK overvejes ved heparin kontraindikation Til højrisiko patienter vurderet ud fra kredsløbspåvirkning og påvirkning af højre ventrikel 2. linie: Højrisiko patienter med kontraindikation for trombolyse konfereres med thoraxkirurger m.h.p. embolektomi

28
DVT/LE (minus cancer) – sekundær profylakse 1
DVT/LE (minus cancer) – sekundær profylakse 1. linie: Alle patienter én af nedenstående behandlinger med varighed afhængig af recidivrisiko VKA NOAK VKA forudsætter, at INR ligger mellem 2 og 3 med et gennemsnitligt TTI på > 70% 2.linie: NOAK Lægemiddelvalg træffes af læge og patient i fællesskab efter samlet individuel vurdering, på baggrund af effekt og bivirkninger, medikamentspecifikke interaktionspotentialer, patientønske og –compliance samt behandlingsvarighed 2.linie: VKA
 – sekundær profylakse 1. linie: Alle patienter én af nedenstående behandlinger med varighed afhængig af recidivrisiko. VKA. NOAK. VKA forudsætter, at INR ligger mellem 2 og 3 med et gennemsnitligt TTI på > 70% 2.linie: NOAK Lægemiddelvalg træffes af læge og patient i fællesskab efter samlet individuel vurdering, på baggrund af effekt og bivirkninger, medikamentspecifikke interaktionspotentialer, patientønske og –compliance samt behandlingsvarighed 2.linie: VKA")
29
DVT/LE (cancer) – sekundær profylakse
1. linie: Dalteparin eller tinzaparin DVT: dalteparin eller tinzaparin LE: dalteparin eller tinzaparin 2.linie: VKA forudsat, at INR ligger mellem 2 og 3 med et gennemsnitligt TTI på > 70%. Alternativt anvendes NOAK.

30
Apopleksi er den mest almindelige men også mest alvorlige komplikation til atrieflimren
AF er hovedårsag til iskæmisk apopleksi hos 15 – 20% af patienterne1 AF øger apopleksi-risikoen med 4 til 5 gange2 AF er en selvstændig risikofaktor for sværhedsgrad og recidivrisiko ved iskæmisk apopleksi3 Apopleksi-risiko ens for asymptomatisk og symptomatisk AF4 1. Go AS. Am J Geriatr Cardiol 2005;14: Wolf PA, et al. Stroke 1991;22: Penado S, et al. Am J Med 2003;114: Page RL, et al. Circulation 2003;107:

32
Prævalens af atrieflimren forventes mindst fordoblet indtil 2050
15.9 Olmsted County data (assuming a continued increase in AF incidence)1,2 16 15.2 14.3 14 13.1 11.7 Olmsted County data (assuming no further increase in AF incidence)1,2 12 10.2 12.1 11.7 10 8.9 11.1 10.3 7.7 Patients with AF (millions) 9.4 8 6.7 8.4 5.9 7.5 6 5.1 ATRIA study data2,3 6.8 6.1 5.6 5.61 4 5.16 5.42 5.1 4.78 4.34 3.80 2 3.33 2.94 2.44 2.66 2.08 2.26 Year 1990 1995 2000 2005 2010 2015 2020 2025 2030 2035 2040 2045 2050 1. Miyasaka Y, et al. Circulation 2006;114: Savelieva I, Camm AJ. Clin Cardiol 2008;31:55-62 3. Go AS, et al. JAMA 2001;285:2370-5 32
1, Olmsted County data (assuming no further increase in AF incidence)1, Patients with AF (millions) ATRIA study data2, Year Miyasaka Y, et al. Circulation 2006;114: Savelieva I, Camm AJ. Clin Cardiol 2008;31: Go AS, et al. JAMA 2001;285:")
33
‘Natural’ time course of AF.
‘Natural’ time course of AF. AF = atrial fibrillation. The dark blue boxes show a typical sequence of periods in AF against a background of sinus rhythm, and illustrate the progression of AF from silent and undiagnosed to paroxysmal and chronic forms, at times symptomatic. The upper bars indicate therapeutic measures that could be pursued. Light blue boxes indicate therapies that have proven effects on ‘hard outcomes’ in AF, such as stroke or acute heart failure. Red boxes indicate therapies that are currently used for symptom relief, but may in the future contribute to reduction of AF-related complications. Rate control (grey box) is valuable for symptom relief and may improve cardiovascular outcomes. Camm A J et al. Eur Heart J 2010;eurheartj.ehq278 33
 is valuable for symptom relief and may improve cardiovascular outcomes. Camm A J et al. Eur Heart J 2010;eurheartj.ehq")
34
Atrieflimren - risikoscore
Number of risk factors Risk of bleeding 1.13 1 1.02 2 1.88 3 3.74 4 8.70 5 12.5 6–9 ?

35
Trials with new agents vs warfarin (INR 2.0-3.0) in AF
RELY ROCKET ARISTOTLE ENGAGE-AF Sample size 18,113 14,266 18,201 20,500 New treatment Dabigatran 110mg BID & 150mg BID Rivaroxaban 20mg QD Apixaban 5mg BID Edoxaban 30mg QD & 60mg QD Design Non-inferiority PROBE Double-blind CHADS2 ≥ 1 ≥ 2 Primary outcome Stroke or systemic embolism Safety outcome Primary: Major Bleeding Connolly S et al NEJM 2009; Patel M et al NEJM 2011; Granger C et al NEJM 2011; ENGAGE- AF Study Investigators. AHJ 2010

37
TTI = 64 % TTI = 62 % TTI = 55 %

38
Dansk vejledning (RADS/DCS)
")
40
Valg af oral antikoagulansbehandling ved atrieflimren (RADS)
Beslutning om initiering af behandling bør ske efter en samlet individuel vurdering af patienten og på baggrund af Effekt Bivirkninger Hensyn til medikament-specifikke interaktionspotentialer Patientønske Generel compliance Valg af behandling træffes på denne baggrund af læge og patient i fællesskab med udgangspunkt i en trombose risikovurdering og vurdering af blødningsrisikoen. Ved valg af vitamin K-antagonist behandling (VKA) skal INR forventeligt ligge mellem 2 og 3 med TTI i ≥ 70%.
 skal INR forventeligt ligge mellem 2 og 3 med TTI i ≥ 70%.")
41
Valg af oral antikoagulansbehandling ved atrieflimren (RADS)
Vurderingsrækkefølge Først vurderes om warfarin ud fra en samlet individuel vurdering samt den behandlingsmæssige kvalitet målt i TTI > 70 % er det rigtige lægemiddelvalg. Hvis ikke warfarin vurderes som et godt lægemiddelvalg, vurderes om det rigtige lægemiddelvalg er rivaroxaban, dabigatran eller apixaban Første vurderings-mulighed: Warfarin, doseres individuelt. Forudsætter at INR er mellem 2 og 3 med et TTI på ≥ 70%. Anden vurderings-mulighed: Uprioriteret Xarelto, rivaroxaban 20 mg x 1 (15 mg x 1) Pradaxa, dabigatran 150 mg x 2 (110 mg x 2) Eliquis, apixaban 5 mg x (2,5 mg x 2 )
 Pradaxa, dabigatran 150 mg x 2 (110 mg x 2) Eliquis, apixaban 5 mg x 2 (2,5 mg x 2 )")
42
Valg af oral antikoagulansbehandling
Efterlevelse Det forventes at langt størstedelen af patienter med non-valvulær atrieflimren vil modtage antikoagulansbehandling i henhold til denne lægemiddelrekommandation. I Region Midt er besluttet, at der ydes fuld refusion af lægemiddeludgifter til afdelinger, der følger RADS anbefalinger vedrørende dyr sygehusmedicin

43
Apixaban 5 mg BD (2.5 mg in selected patients)
AVERROES AVERROES: Apixaban in patients with atrial fibrillation who have failed or are unsuitable for VKA treatment Event-driven N=5,599 Aspirin 81–324 mg OD Apixaban 5 mg BD (2.5 mg in selected patients) Patient Population Patients with AF and one or more risk factors for stroke Not receiving VKA therapy (demonstrated or expected to be unsuitable for VKA) Primary Outcomes Confirmed ischaemic stroke, haemorrhagic stroke, or systemic embolism Secondary Outcomes Confirmed ischaemic stroke, haemorrhagic stroke, systemic embolism, myocardial infarction, or vascular death 522 centres AVERROES=Apixaban VERsus Acetylsalicylic Acid (ASA) to PRevent StrOkES. Connolly SJ et al. N Engl J Med. 2011;364:806–817 Eikelboom JW et al. Am Heart J 2010;159:348–353.e1. Eikelboom JW, O’Donnell M, Yusuf S, et al. Rationale and design of AVERROES: apixaban versus acetylsalicylic acid to prevent stroke in atrial fibrillation patients who have failed or are unsuitable for vitamin K antagonist treatment. Am Heart J. 2010;159: e1. 43
 Patient Population. Patients with AF and one or more risk factors for stroke. Not receiving VKA therapy (demonstrated or expected to be unsuitable for VKA) Primary Outcomes. Confirmed ischaemic stroke, haemorrhagic stroke, or systemic embolism. Secondary Outcomes. Confirmed ischaemic stroke, haemorrhagic stroke, systemic embolism, myocardial infarction, or vascular death. 522 centres. AVERROES=Apixaban VERsus Acetylsalicylic Acid (ASA) to PRevent StrOkES. Connolly SJ et al. N Engl J Med. 2011;364:806–817. Eikelboom JW et al. Am Heart J 2010;159:348–353.e1. Eikelboom JW, O’Donnell M, Yusuf S, et al. Rationale and design of AVERROES: apixaban versus acetylsalicylic acid to prevent stroke in atrial fibrillation patients who have failed or are unsuitable for vitamin K antagonist treatment. Am Heart J. 2010;159: e")
44
Stroke or systemic embolism
AVERROES Stroke or systemic embolism Hazard ratio with apixaban, 0.45 (95% CI, 0.32–0.62) p<0.001 0.05 Aspirin 0.04 0.03 Cumulative Hazard 0.02 Apixaban 0.01 0.00 3 6 9 12 18 Time (months) No. at Risk Aspirin 2791 2716 2530 2112 1543 628 Apixaban 2808 2758 2566 2125 1522 615 44 Adapted from Connolly SJ et al. N Engl J Med 2011;364:806–817 Connolly SJ, Eikelboom J, Joyner C, et al, for the AVERROES Steering Committee and Investigators. Apixaban in patients with atrial fibrillation. N Engl J Med. 2011; /NEJMoa 44 44
 p< Aspirin Cumulative Hazard Apixaban Time (months) No. at Risk. Aspirin Apixaban Adapted from Connolly SJ et al. N Engl J Med 2011;364:806–817. Connolly SJ, Eikelboom J, Joyner C, et al, for the AVERROES Steering Committee and Investigators. Apixaban in patients with atrial fibrillation. N Engl J Med. 2011; /NEJMoa")
45
Hazard ratio with apixaban, 1.13 (95% CI, 0.74–1.75)
AVERROES Major bleeding Hazard ratio with apixaban, 1.13 (95% CI, 0.74–1.75) 0.020 p=0.57 Apixaban 0.015 Aspirin Cumulative hazard 0.010 0.005 0.00 3 6 9 12 18 Time (months) No. at Risk Aspirin 2791 2738 2557 2140 1571 642 Apixaban 2808 2759 2566 2120 1521 622 CI, confidence interval Adapted from Connolly SJ et al. N Engl J Med 2011;364:806–817 Connolly SJ, Eikelboom J, Joyner C, et al, for the AVERROES Steering Committee and Investigators. Apixaban in patients with atrial fibrillation. N Engl J Med. 2011; /NEJMoa 45
 p=0.57. Apixaban Aspirin. Cumulative hazard Time (months) No. at Risk. Aspirin Apixaban CI, confidence interval. Adapted from Connolly SJ et al. N Engl J Med 2011;364:806–817. Connolly SJ, Eikelboom J, Joyner C, et al, for the AVERROES Steering Committee and Investigators. Apixaban in patients with atrial fibrillation. N Engl J Med. 2011; /NEJMoa")
46
Antitrombotisk behandling ved akut koronart syndrom
46

47
2014 ACS Treatment Recommendations
ECG, troponin ASA + ADP-reeptor blocker β-blocker + nitrate Persistent ST-segment elevation Primary PCI or fibrinolysis High risk Coronary angiography urgent PCI / CABG No persistent ST-segment elevation + LMWH / UFH / fondaparinux / bivalirudin Intermediate risk Coronary angiography 1-3 days ASA+ADP-receptor blocker + β-blocker + statin + ACE inhibitor Pos Low risk Stress test ASA (+ statin) Neg ACE = angiotensin-converting enzyme; ACS = acute coronary syndromes; ASA = acetylsalicylic acid; CABG = coronary artery bypass graft; ECG = electrocardiogram; GP = glycoprotein; LMWH = low-molecular-weight heparin; PCI = percutaneous coronary intervention; UFH = unfractionated heparin. 47 47
 Neg. ACE = angiotensin-converting enzyme; ACS = acute coronary syndromes; ASA = acetylsalicylic acid; CABG = coronary artery bypass graft; ECG = electrocardiogram; GP = glycoprotein; LMWH = low-molecular-weight heparin; PCI = percutaneous coronary intervention; UFH = unfractionated heparin")
48
Akut koronart syndrom: ± PCI
Kontakt til sundhedsvæsen Dual trombocythæmning + PCI EKG Pt får brystsmerter 12 mdr. dual trombocythæmning - PCI

49
Hvilken ADP-receptor blokker er bedst eller er der ligeværdige alternativer ??
49

50
Standard behandling fra 2001-2009: ASA + clopidogrel
Nye muligheder siden 2009/2010: ASA + prasugrel (Efient) ASA + ticagrelor (Brilique) 50
 ASA + ticagrelor (Brilique)")
51
Prasugrel (Efient) kun godkendt til PCI pts.
12 mdr. dual trombocythæmning PPCI Kontakt til sundhedsvæsen Dual trombocythæmning EKG Pt får brystsmerter KAG/PCI < 48 timer Hjemstedssgh 12 mdr. dual trombocythæmning

52
Direkte sammenlignende RCT
Clopidogrel+ASA versus Efient+ASA (TRITON-TIMI 38) Clopidogrel+ASA versus Brilique+ASA (PLATO) Ingen direkte sammenlignende RCT 52
 Clopidogrel+ASA versus Brilique+ASA (PLATO) Ingen direkte sammenlignende RCT. 52.")
53
Efient+ASA versus clopidogrel+ASA: Forskel i patientrelevante hændelser efter 1 års behandling.
Effekt af ASA+PRA versus ASA+CLO (hos patienter med nyligt AKS og PCI) Vaskulær mortalitet Ingen signifikant effekt Nonfatal MI 16 færre tilfælde pr behandlede Stroke omfattende nonfatal iskæmisk og hæmoragisk stroke Major ekstrakranielle blødninger 11 flere tilfælde pr behandlede 53
 Vaskulær mortalitet. Ingen signifikant effekt. Nonfatal MI. 16 færre tilfælde pr behandlede. Stroke omfattende nonfatal iskæmisk og hæmoragisk stroke. Major ekstrakranielle blødninger. 11 flere tilfælde pr behandlede")
54
Brilique+ASA versus clopidogrel+ASA: Forskel i patientrelevante hændelser efter 1 års behandling.
Effekt af ASA+TICA versus ASA+CLO (hos patienter med nyligt AKS) Vaskulær mortalitet 10 færre tilfælde pr behandlede Nonfatal MI 11 færre tilfælde pr behandlede Stroke omfattende nonfatal iskæmisk og hæmoragisk stroke Ingen signifikant effekt Major ekstrakranielle blødninger 6 flere tilfælde pr behandlede 54
 Vaskulær mortalitet. 10 færre tilfælde pr behandlede. Nonfatal MI. 11 færre tilfælde pr behandlede. Stroke omfattende nonfatal iskæmisk og hæmoragisk stroke. Ingen signifikant effekt. Major ekstrakranielle blødninger. 6 flere tilfælde pr behandlede")
55
Konklusion 1 Efient og Brilique er bedre end clopidogrel. 08-04-2017
55

56
Efient versus Brilique
10 færre dødsfald 11 færre myokardieinfarkter, 6 ekstra tilfælde af major ekstrakranielle blødninger Er bedre end 17 færre myokardieinfarkter 7 ekstra tilfælde af major ekstrakranielle blødninger 56

57
Akut koronart syndrom: ± PCI
Kontakt til sundhedsvæsen Dual trombocythæmning + PCI EKG Pt får brystsmerter 12 mdr. dual trombocythæmning - PCI

58
Simplet regime ved AKS Dual trombocythæmning i 12 mdr
Kontakt til sundhedsvæsen EKG Pt får brystsmerter

59
Fagudvalgets anbefaling: ASA+Brilique til AKS
Dual trombocythæmning i 12 mdr Kontakt til sundhedsvæsen EKG Pt får brystsmerter

60
Risk of bleeding - MI (n = 40,812)
Lancet, Dec. 12, 2009

61
Adjusted risk Cox proportional hazard model
Non-fatal and fatal bleeding NNH Reference 115.7 165.9 81.2 45.2 15.2 12.5 Som anførte først varierer baseline for de enkelte expoure groups, men når man laver anlysere i en COX model med Exposure groups som tidsafhængige variables ses tendens stadig, hvilket den også gør i en række sensitivitets analyser Bleeding 3-times augmented risk for death or re-MI Sørensen et al, The Lancet, Dec 12-18,2009 61

62
WOEST trial - RCT 1 2 Patients with VKA PCI/ACS, n=563
Randomized to: Endpoints: Bleeding Combined: stroke, re-MI, TVR, stent thrombosis, mortality 1 VKA+clopidogrel 2 VKA+clopidogrel+aspirin Dewilde et al, the Lancet, Feb 13th, 2013 62

63
WOEST trial - bleeding Dewilde et al, the Lancet, Feb 13th, 2013 63

64
WOEST trial - MACE Combined: Death, MI, TVR, stroke, stent-thrombosis
Dewilde et al, the Lancet, Feb 13th, 2013

65
European joint consensus: Choice of antithrombotic therapy
References: 1. Lip et al. EHJ 2014 (epub) *Dual therapy with OAC and clopidogrel may be considered in selected patients. **ASA as an alternative to clopidogrel may be considered in patients on dual therapy (i.e. OAC plus single antiplatelet). ***Dual therapy with OAC and an antiplatelet agent (ASA or clopidogrel) may be considered in patients at very high risk of coronary events 1. Lip et al. Eur Heart J 2014 (epub) 65
 *Dual therapy with OAC and clopidogrel may be considered in selected patients. **ASA as an alternative to clopidogrel may be considered in patients on dual therapy (i.e. OAC plus single antiplatelet). ***Dual therapy with OAC and an antiplatelet agent (ASA or clopidogrel) may be considered in patients at very high risk of coronary events. 1. Lip et al. Eur Heart J 2014 (epub) 65.")
66
Conclusions Patients with AF who suffer an ACS and undergo PCI frequently receive triple antithrombotic therapy, despite the increased risk of bleeding1 The WOEST trial indicates that ASA therapy may not be necessary in these patients2 Joint consensus opinion recommends that antithrombotic strategy is based upon stroke and bleeding risk1 Joint consensus opinion recommends that either a NOAC or warfarin can be used as anticoagulant1 Joint consensus opinion recommends that ticagrelor and prasugrel should not be used together with oral anticoagulation1 Abbreviations ACS, acute coronary syndrome; AF, atrial fibrillation; ASA, acetylsalicylic acid; NOAC, novel oral anticoagulant; PCI, percutaneous coronary intervention; WOEST, What is the Optimal Antiplatelet and Anticoagulant Therapy in Patients with Oral Anticoagulation and Coronary Stenting References 1. Lip et al. Eur Heart J 2014 (epub) 2. DeWilde et al. Lancet :1107–1115 3. 4. 1. Lip et al, 2014; 2. DeWilde et al, 2013; 66
 2. DeWilde et al. Lancet :1107– Lip et al, 2014; 2. DeWilde et al, 2013;")
Lignende præsentationer










 (Nyt program - 1. september) LifePak ® (eksempel) – 72,40 PSV 401,60 DKK med 5 % rabat= 381,52 DKK (68,78 PSV) Fragt.>")












