Download præsentationen
Præsentation er lastning. Vent venligst

1
Dyspepsi IRF 26. januar 2010 Læge, ph.d, Christina Reimer

2
Behandling og behandlingsvarighed
Ulcus Profylakse Funktionel Dyspepsi Gastroesophageal Reflux Sygdom

3
A02 Midler mod syrerelaterede forstyrrelser
Antacida H2-receptor antagonister Prostaglandiner Protonpumpehæmmere Andre midler (sucralfat, alginsyre)
")
4
Ulcus sygdom H. pylori ASA/NSAIDs

5
Ulcus ætiologi Reimer et al, Scand J Gastroenterology 2008

6
Behandling og behandlingsvarighed ved H. pylori positivt ulcus
PPI i standarddosis x 2 dagligt Clarithromycin 500 mg x 2 dagligt Amoxicillin 1 g x 2 dagligt Behandlingsvarighed: 7 dage Ved større ulcera suppleres med PPI behandling i 2-4 uger H.Pylori test 4-6 uger efter kur Positiv H. pylori test

7
Faktorer af betydning for vellykket eradikationsbehandling
Compliance (ignorer bivirkninger!) Resistensmønster - Metronidazol 30% - Clarithromycin < 10% - Amoxicillin 0% Test 4-6 uger efter afsluttet kur
 Resistensmønster. - Metronidazol 30% - Clarithromycin < 10% - Amoxicillin 0% Test 4-6 uger efter afsluttet kur.")
8
Behandling og behandlingsvarighed ved NSAID/ASA associeret ulcus
Seponer ASA/NSAID PPI i standard dosis i 4-8 uger Negativ H. pylori test Oplysninger om forbrug af ASA/NSAID

9
Ved gentagne mislykkede forsøg på Helicobacter pylori-eradikation
Hvornår er vedligeholdelsesbehandling med syrepumpehæmmer (PPI) efter ulcusheling indiceret? Ved recidiverende ulcera, trods Helicobacter pylori-negativ test (idiopatisk ulcus) Ved gentagne mislykkede forsøg på Helicobacter pylori-eradikation Ved fortsat indikation for ASA/NSAID-behandling. Klinisk vejledning: Udredning og behandling af dyspepsi. DSAM 2009
 efter ulcusheling indiceret Ved recidiverende ulcera, trods Helicobacter pylori-negativ test (idiopatisk ulcus) Ved gentagne mislykkede forsøg på Helicobacter pylori-eradikation. Ved fortsat indikation for ASA/NSAID-behandling. Klinisk vejledning: Udredning og behandling af dyspepsi. DSAM")
10
Hvordan forebygges ASA/NSAID-relaterede ulcuskomplikationer?
Genovervej indikationen for ASA/NSAID-behandling Vurder patientens risiko for ulcus-komplikation: Alder (risiko er stigende med alder, specielt > 60 år) Tidligere ulcus Tidligere ulcusblødning/perforation Dyspepsi Anden sygdom (diabetes, hjerte-kar-sygdom eller svær kronisk leddegigt) Samtidig behandling med steroid, SSRI eller AK-behandling
 Tidligere ulcus. Tidligere ulcusblødning/perforation. Dyspepsi. Anden sygdom (diabetes, hjerte-kar-sygdom eller svær kronisk leddegigt) Samtidig behandling med steroid, SSRI eller AK-behandling.")
11
Ofte er risikoen åbenlys

12
Gastroskopien var normal…….
Behandling af funktionel dyspepsi Det kommer af græsk Hva´ kommer dyspepsi af?

13
Medikamentel behandling af funktionel dyspepsi
Stort placebo respons H2RA og PPI hjælper kun få (10-15%) Ingen indikation for antacida Ringe symptomatisk effekt af eradikation (NNT = 15) Beroligelse og information om tilstandens godartede natur hjælper
 Ingen indikation for antacida. Ringe symptomatisk effekt af eradikation (NNT = 15) Beroligelse og information om tilstandens godartede natur hjælper.")
14
Overlap af symptomer fra fra øvre mave-tarm kanal
Dyspepsi Reflux symptomer

15
Refluks pyramiden Adenocarcinom Barrett og komplikationer Svær erosiv
Mild erosiv NERD

16
Forskellige former for GERD
≥60% ~35% <5% Non-Erosiv Reflukssygdom Erosiv Oesophagitis Barrett’s Oesophagus Non-progressiv Normal endoskopi Striktur Ulcus GI blødning Adenocarcinom i oesophagus

17
Virker livsstilmodifikationer ved GERD?
Vægttab Effektivt Ligge højt med hovedet Effektivt Rygeophør Ingen evidens Ophør med alkohol Ingen evidens Kostændring Ingen evidens Kaltenbach et al. Arch Intern Med 166: (2006)
")
18
Medicinsk behandling? Patienter med komplikationer til GERD (erosioner, ulceration, striktur, Barretts øsofagus) og patienter som oplever nedsat livskvalitet som følge af symptomerne bør tilbydes medicinsk behandling Patienter med milde og sporadiske symptomer kan behandles med antacida og H2-blokker Ved svære og hyppige symptomer behandles med syrepumpehæmmer i standarddosis
 og patienter som oplever nedsat livskvalitet som følge af symptomerne bør tilbydes medicinsk behandling. Patienter med milde og sporadiske symptomer kan behandles med antacida og H2-blokker. Ved svære og hyppige symptomer behandles med syrepumpehæmmer i standarddosis.")
19
Almost all GERD patients relapse after treatment discontinuation
Relapsed % 100 80 60 Severe (Grade C) 40 Moderate (Grade B) Mild (Grade A) 20 No esophagitis 1 2 3 4 5 6 Time (months) Lundell et al. Gut 45:172–80 (1999)
 40. Moderate (Grade B) Mild (Grade A) 20. No esophagitis Time (months) Lundell et al. Gut 45:172–80 (1999)")
20
Treatment options in GERD
Continuous maintenance (months–years) Intermittent courses (weeks) S On-demand (days) S S = symptom recurrence
 Intermittent courses (weeks) S. On-demand (days) S. S = symptom recurrence.")
21
Mild reflux esophagitis Severe reflux esophagitis
Endoscopy Normal endoscopy NERD Mild reflux esophagitis Severe reflux esophagitis PPI (4)–8 weeks Success: continuous PPI Bytzer P, Blum AL. Aliment Pharmacol Ther 20:389–98 (2004)
–8 weeks. Success: continuous PPI. Bytzer P, Blum AL. Aliment Pharmacol Ther 20:389–98 (2004)")
22
Mild reflux esophagitis Severe reflux esophagitis
Endoscopy Normal endoscopy NERD Mild reflux esophagitis Severe reflux esophagitis PPI (2)–4 weeks Success: continuous/ on-demand PPI Bytzer & Blum, Aliment Pharmacol Ther 20:389–98 (2004)
–4 weeks. Success: continuous/ on-demand PPI. Bytzer & Blum, Aliment Pharmacol Ther 20:389–98 (2004)")
23
Mild reflux esophagitis Severe reflux esophagitis
Endoscopy Mild reflux esophagitis Severe reflux esophagitis NERD PPI weeks Success: Consider on demand or continuous PPI Bytzer & Blum, Aliment Pharmacol Ther 20:389–98 (2004)
")
24
Heling proportional med syrehæmning
Heling af øsofagit (%) 100 PPI 80 60 H2-receptor antagonister PPIs and H2-receptor antagonists in healing esophagitis. As PPIs are able to maintain the intraesophageal pH at 4 or above for longer, they are more effective in healing esophagitis compared with H2-receptor antagonists. This figure shows a meta-analysis of randomised, single- or double-blind clinical trials conducted in patients with GERD with endoscopically proven erosive or ulcerative esophagitis. The meta-analysis incorporated a total of 43 studies involving 7635 patients treated for 2–12 weeks. For all time points between 2 and 12 weeks, the mean percentage of patients in whom esophagitis was healed was considerably higher with PPIs than with H2-receptor antagonists. Notably, the same proportion of patients were healed after 2 weeks with PPIs (63.4%) as were healed after 12 weeks with H2-receptor antagonists (60.2%). The overall proportion of cases healed, regardless of the duration of treatment, was 83.6% with PPIs, 51.9% with H2-receptor antagonists and 28.2% with placebo (p< between groups). 40 placebo 20 2 4 6 8 10 12 Tid (uger) Chiba et al 1997
 100. PPI H2-receptor antagonister. PPIs and H2-receptor antagonists in healing esophagitis. As PPIs are able to maintain the intraesophageal pH at 4 or above for longer, they are more effective in healing esophagitis compared with H2-receptor antagonists. This figure shows a meta-analysis of randomised, single- or double-blind clinical trials conducted in patients with GERD with endoscopically proven erosive or ulcerative esophagitis. The meta-analysis incorporated a total of 43 studies involving 7635 patients treated for 2–12 weeks. For all time points between 2 and 12 weeks, the mean percentage of patients in whom esophagitis was healed was considerably higher with PPIs than with H2-receptor antagonists. Notably, the same proportion of patients were healed after 2 weeks with PPIs (63.4%) as were healed after 12 weeks with H2-receptor antagonists (60.2%). The overall proportion of cases healed, regardless of the duration of treatment, was 83.6% with PPIs, 51.9% with H2-receptor antagonists and 28.2% with placebo (p< between groups). 40. placebo Tid (uger) Chiba et al")
25
Opsamling Behandling af ulcussygdommen er i størstedelen af tilfældene kortvarig (4-8 uger) Længerevarende fast behandling med PPI er indiceret ved erosiv reflukssygdom og som profylakse mod ASA/NSAID-relaterede ulcuskomplikationer

26
Opsamling Langtids-PPI-behandling af NERD kan ofte være symptomstyret efter on-demand principperne Ved behandling af funktionel dyspepsi er der kun evidens for en beskeden effekt af syrehæmmende behandling i kortere tid P.g.a højt placeborespons og stort symptomoverlap må langtids-PPI-behandling baseret på symptomer evalueres kritisk og følges af regelmæssige seponeringsforsøg

27
PPIs on prescription Use in DDD/1000 inhabitants per day
Danish Medicines Agency. Medicinal Product Statistics 2008

29
Long-term use of PPIs in primary care in Denmark
22 GP’s with a total of registered pts. Standardized search for prescription of PPIs in each practice prescribing register Patients who had prescriptions of ≥120 tablets in previous year defined as long-term users Indications for long-term therapy ascertained by reviewing records for results of endoscopy, H. pylori testing, pH-monitoring and clincal assesment by the GP

30
Reasons for PPI therapy
Verified indications Treatment based on symptoms Investigated without findings Non-erosive reflux disease (NERD) Functional dyspepsia Endoscopically documented GERD Unexplained or NSAID/ASA induced peptic ulcer or GI bleed Uninvestigated Empirical therapy of upper GI sxs
 Functional dyspepsia. Endoscopically. documented GERD. Unexplained or. NSAID/ASA induced. peptic ulcer or GI. bleed. Uninvestigated. Empirical therapy of upper GI sxs.")
31
Prevalence of long-term PPI therapy
5.3% (2.275/42.634) had at least one PPI prescription 2.1% (901/42.634) were long-term treated (≥120 tablets/previous year) Verified indication 27% (247/901) Treated based on symptoms 73% (654/901) Reimer et al. Aliment pharm and ther. 2009
 had at least one PPI prescription. 2.1% (901/42.634) were long-term treated. (≥120 tablets/previous year) Verified indication. 27% (247/901) Treated based on symptoms. 73% (654/901) Reimer et al. Aliment pharm and ther")
32
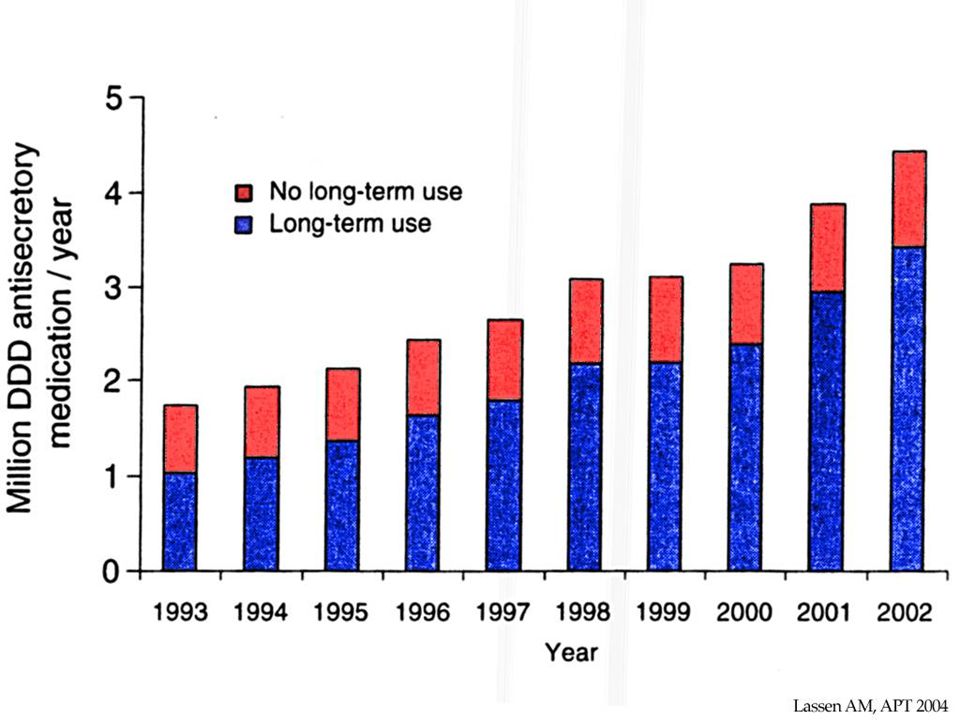
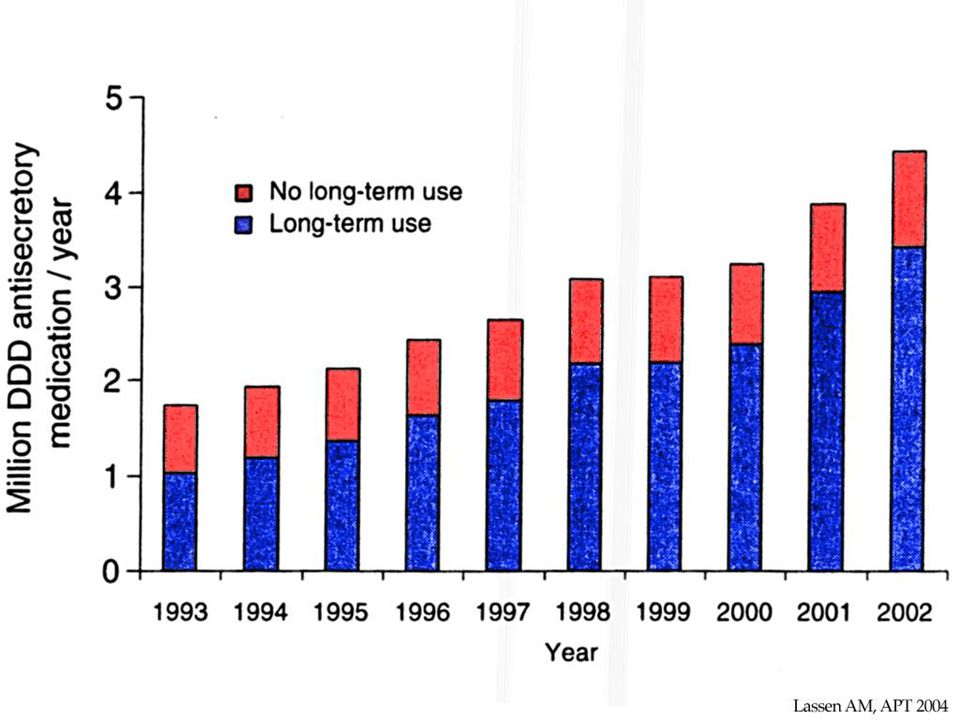
Indications and reasons for long-term PPI therapy (N=901)
Reimer et al. Aliment pharm and ther. 2009

33
Self-reported characteristics of patients long-term treated based on symptoms (n=194)
")
35
Maximal acid output in 12 H
Maximal acid output in 12 H.pylori-negative subjects before, during and after 8 weeks treatment with a PPI mmol/h Gillen, Gastroenterology 2004;126:

36
Treatment with a PPI for at least 8 weeks induces rebound acid hypersecretion (RAHS) after therapy has been discontinued in H.pylori negative individuals It sets off 1-2 weeks after therapy is withdrawn and is a temporary phenomenon Is it clinically relevant? Could this phenomenon provoke acid-related symptoms and thus lead to PPI dependency?

37
Placebo 120 healthy volunteers Esomeprazole 40 mg od Placebo Week Week 0,1,2,3,4,5,6,7,8,9,10,11,12: GSRS (Gastrointestinal Symptom Rating Scale) Week 0, 4, 8, 12: Gastrin, Chromogranin A (CgA)
 Week 0, 4, 8, 12: Gastrin, Chromogranin A (CgA)")
38
Outcome measures 1. Have you been bothered by stomach ache or pain in the upper abdomen during the past week? 2. Have you been bothered by heartburn during the past week? 3. Have you been bothered by acid reflux during the past week? (1) No discomfort at all (2) Slight discomfort (3) Mild discomfort (4) Moderate discomfort (5) Moderately severe discomfort (6) Severe discomfort (7) Very severe discomfort Randomisation Placebo Esomeprazole 40 mg x placebo
 No discomfort at all. (2) Slight discomfort. (3) Mild discomfort. (4) Moderate discomfort. (5) Moderately severe discomfort. (6) Severe discomfort. (7) Very severe discomfort. Randomisation. Placebo. Esomeprazole 40 mg x 1 placebo")
39
Mean GSRS score for dyspepsia, heartburn and regurgitation
Reimer et al. Gastroenterology 2009

40
Proportion with score >2 for dyspepsia, heartburn or regurgitation
Reimer et al. Gastroenterology 2009

41
Conclusions Acid inhibition with a PPI for 8 weeks induces acid-related symptoms in a significant proportion (44%) of previously asymptomatic subjects when therapy is withdrawn The most likely underlying explanation is RAHS PPI dependency as one of the explanations for the prevalent and increasing long-term use of PPIs is supported by this study
 of previously asymptomatic subjects when therapy is withdrawn. The most likely underlying explanation is RAHS. PPI dependency as one of the explanations for the prevalent and increasing long-term use of PPIs is supported by this study.")
42
Implications Rationalisation of PPI prescribing can be obtained in subgroups of patients treated long-term based on symptoms only In patients who are treated based on unspecific symptoms that are not likely to be acid-related, a short course of empirical therapy is important in order to avoid inducing true acid-related symptoms caused by RAHS Otherwise induction of a true need for PPIs in patients with a questionable indication for therapy in the first place is risked

Lignende præsentationer