Download præsentationen
Præsentation er lastning. Vent venligst

1
Diabetisk Ketoacidose Ole Hother-Nielsen Onsdagsundervisning 2015-10-21

2
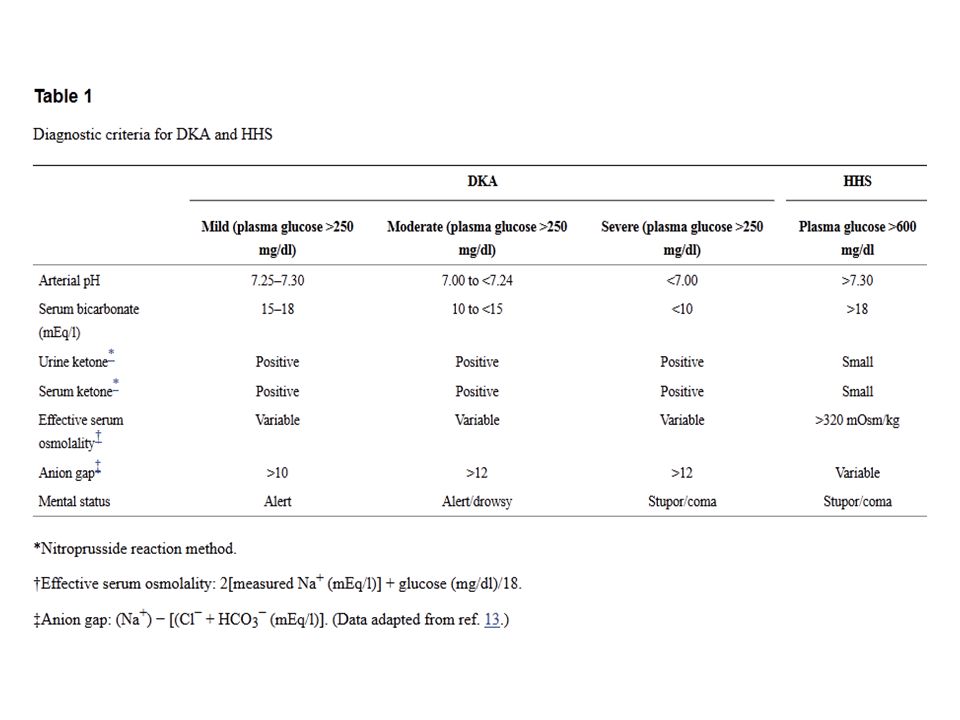
Kitabchi et al. Diabetes Care 2009; 32: 1335

5
Diabetic Ketoacidosis (DKA) P-Glucose (mg/dl) >250 ~ (>13.8 mM) (oftest 30-40 mM) A-pH <7.30 (normal 7.35-7.45) S-Bicarbonate < 15 - 18 mEq/l B-Ketoner (hydroxybutyrat) > 3 mmol/l Urin-ketoner +++ ? (B-Ketoner normalt <0.6mM, faste 0.6-3.0mM, (Abbott: B-Ketoner 16mM OBS begyndende DKA)
.")
6
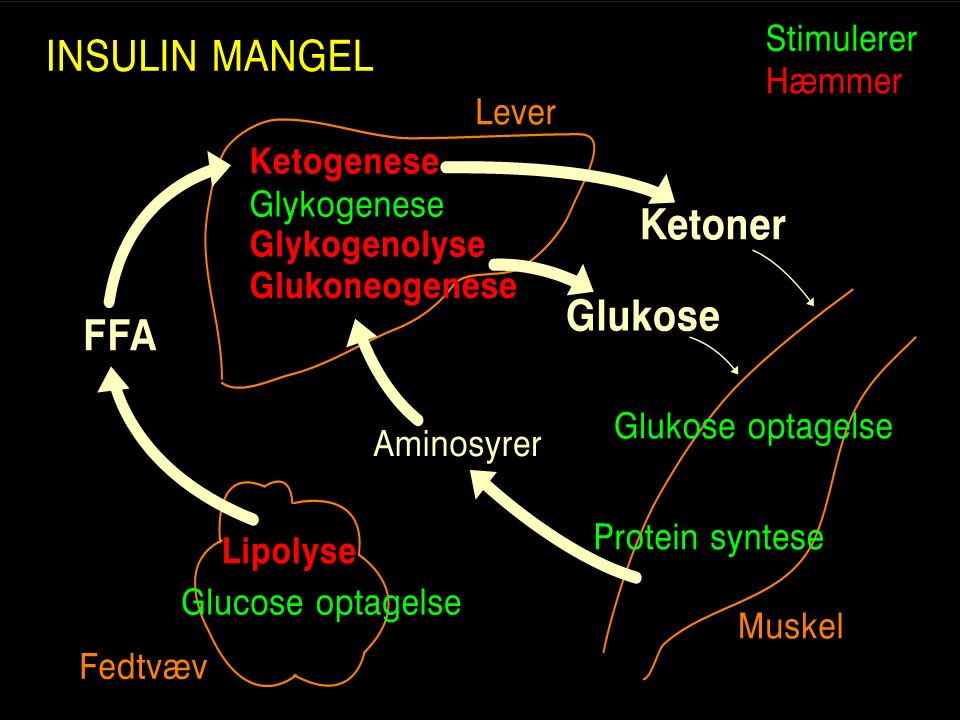
B-Ketone måler beta-hydroxybutyrat i intervallet 0 – 8 mmol/l Ved DKA er Beta-hydroxybutyrat mere forhøjet end acetoacetat

8
Kitabchi et al. Diabetes Care 2009; 32: 1335

9
Ness-Otunnu & Hack. J Emer Med 2013; 45: 797

10
Mortality in DKA 90 % Before discovery of insulin 50 % After discovery of insulin 20 % Antibiotics and forced hydration <10 % 1950s with High-dose insulin regimens < 2 % Resently. Standardized written guidelines Incidens af DKA i USA ca. 15/1000 per yr, sv.t. 300-600 DKA/yr in DK (20.000-40.000 DM-1)
.")
11
Shortly after the introduction of insulin, patients with diabetic coma were treated with 20- 100 units s.c. soluble insulin every 30 min on a sliding scale according to the Benedict test for glucosuria. The total insulin dose for treatment of diabetic coma was increased in the 1940s after the reports by Root (66) and Black and Malins (67), who recommended an initial bolus dose of 200-400 units i.v. Soluble insulin depending on the severity of the mental status. Followed by 50 units i.v. Every 30 min Pasquel. Diabetes Care 2014; 37: 3124
 and Black and Malins (67), who recommended an initial bolus dose of units i.v. Soluble insulin depending on the severity of the mental status. Followed by 50 units i.v. Every 30 min Pasquel. Diabetes Care 2014; 37:")
12
From 1950 to the 1970s, most experts in the field recommended an initial bolus dose of 20-80-units i.m. Or i.v. Followed by 20-80 units i.m. or i.v. Every 1-2 hour. In 1973 Alberti et al. Were the first to report the successful treatment of patients with diabetic coma using smal intramuscular doses of regular insulin. (14 patients, mean bolus 16+2 units, followed by 5-10 units i.v. or i.m. every hour.

14
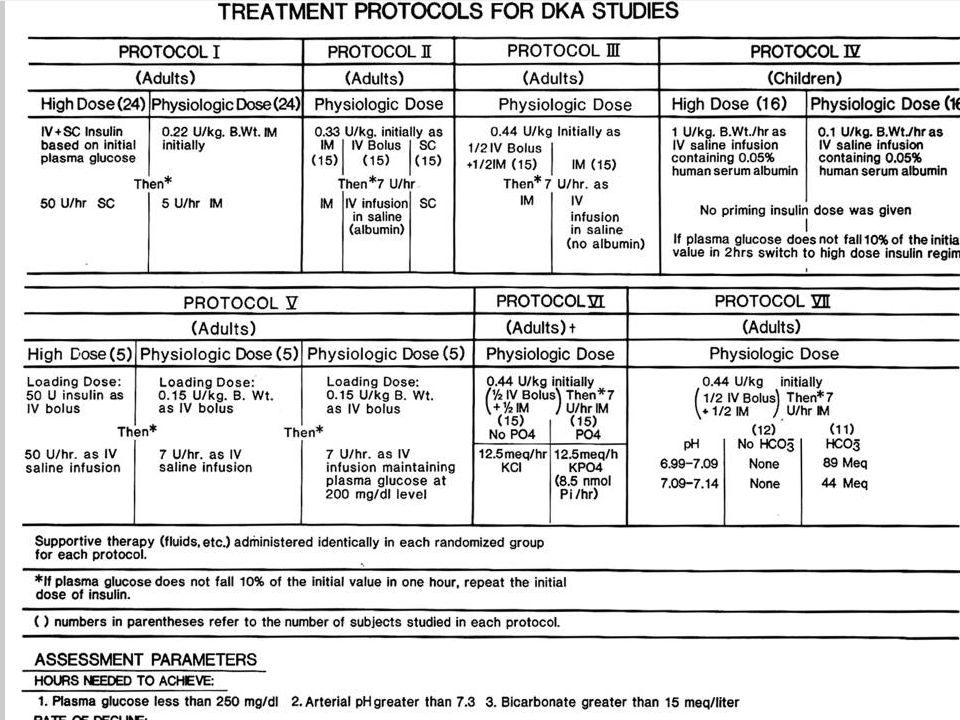
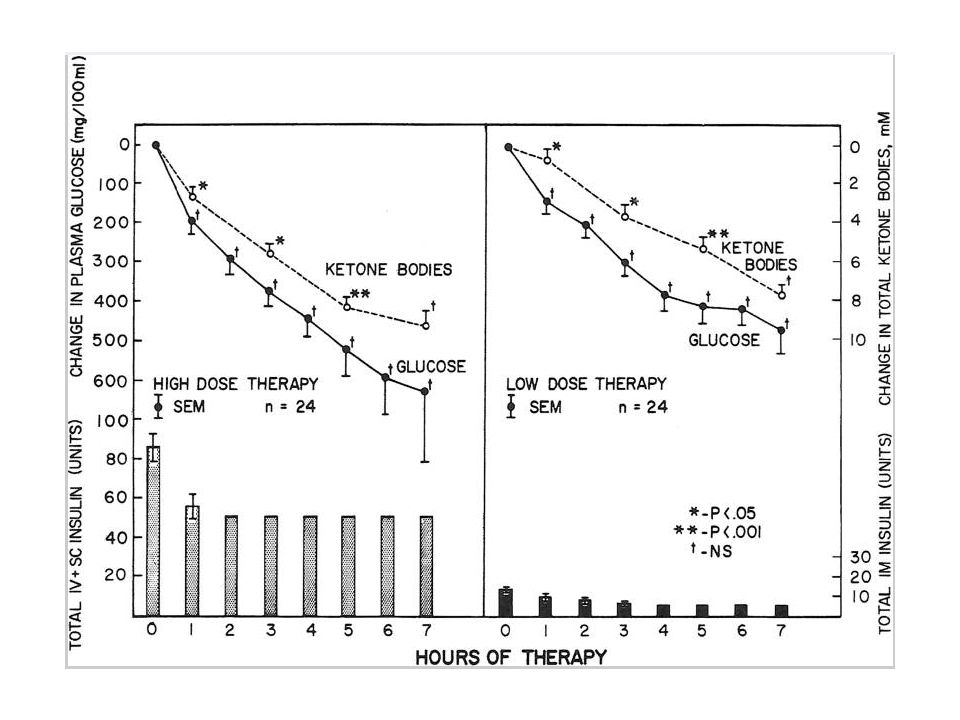
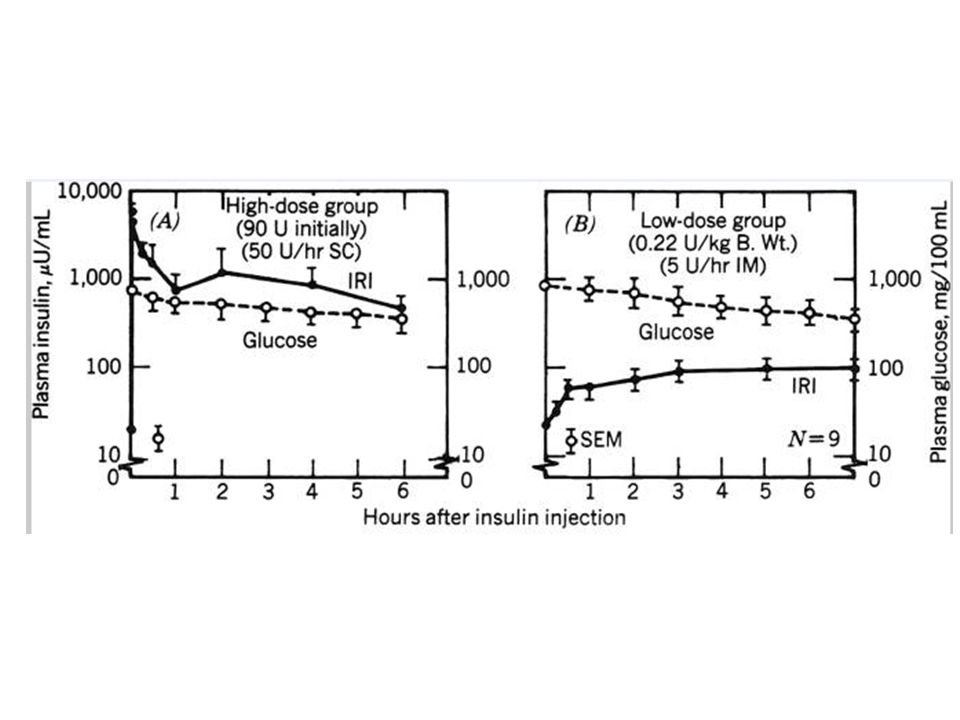
1. High-dose vs Low-dose insulin in Adult DKA 1974 -75 48 patients with DKA – GCRC – (24 + 24) randomiced to High-dose insulin: prime 10-50 U i.v. + 30-100 U s.c. Depending on B-glucose level, followed by 50 U s.c. per hour. Resulting in pharmacological insulin levels of 800-1000 uU/ml. Low-dose insulin: prime 0,22 U/kg i.m. (15 U/70 kg) followed by 5 U/h i.m. Resulting in physiological insulin levels 60-100 uU/ml Time to B-glucose 7,3, and Bicarbonate = 15 mM were not different. But both the incidence of hypoglycemia (25% vs 0%), and of hypokalemia (7/24 vs 1/24) was higher in the high-dose group.
 randomiced to High-dose insulin: prime U i.v U s.c. Depending on B-glucose level, followed by 50 U s.c. per hour. Resulting in pharmacological insulin levels of uU/ml. Low-dose insulin: prime 0,22 U/kg i.m. (15 U/70 kg) followed by 5 U/h i.m. Resulting in physiological insulin levels uU/ml Time to B-glucose 7,3, and Bicarbonate = 15 mM were not different. But both the incidence of hypoglycemia (25% vs 0%), and of hypokalemia (7/24 vs 1/24) was higher in the high-dose group..")
17
2. Route of insulin administration 45 patients with DKA – GCRC – (15 + 15 + 15) were randomized to: intravenous i.v., intramuscular i.m. or subcutaneous s.c. insulin administration. Prime 0,33U/kg followed by 7U/h. Intravenous insulin resulted in higher initial insulin levels (minutes) and greater initial fall in glucose and ketones (first 2 hours) but not thereafter.
 were randomized to: intravenous i.v., intramuscular i.m. or subcutaneous s.c. insulin administration. Prime 0,33U/kg followed by 7U/h. Intravenous insulin resulted in higher initial insulin levels (minutes) and greater initial fall in glucose and ketones (first 2 hours) but not thereafter..")
18
Route of insulin administrations Insulin and glucose levels during: s.c. (upper panel) i.v. (middle) and i.m. (lower panel
 i.v. (middle) and i.m. (lower panel.")
19
2. Route of insulin administration Levels of glucose _____ and ketone bodies ----- during:

20
3. Other Findings A)Mental status on amission was related to serum osmolality, glucose level and age, but not to plasma pH, bicarbonate or ketone bodies. B)It was not necessary to ad albumin to insulin infusates in i.v. Insulin infusions C)Phosphate infusion in DKA had no beneficial effect, but may precipitate hypocalcemia. D)Bicarbonate therapy in DKA is contoversial. Prospective randomized studies showed no beneficial effect in patients with pH > 6.9. Beneficial effect for pH < 6,9 ?? E)Low-dose insulin significantly reduce triglyceride, but not cholesterol levels
Mental status on amission was related to serum osmolality, glucose level and age, but not to plasma pH, bicarbonate or ketone bodies. B)It was not necessary to ad albumin to insulin infusates in i.v. Insulin infusions C)Phosphate infusion in DKA had no beneficial effect, but may precipitate hypocalcemia. D)Bicarbonate therapy in DKA is contoversial. Prospective randomized studies showed no beneficial effect in patients with pH > 6.9. Beneficial effect for pH < 6,9 . E)Low-dose insulin significantly reduce triglyceride, but not cholesterol levels.")
21
Diabetisk ketoacidose Nyopdaget diabetes Kendt diabetes 1) Interkurrent sygdom 2) Mangelfuld insulin tilførsel Årsager
 Interkurrent sygdom 2) Mangelfuld insulin tilførsel Årsager")
22
Diabetisk ketoacidose 1. Akut indlæggelse (alm. Vs intensiv) 2. Ketoacidose regime Insulin Væske og elektrolytter evt. bicarbonat evt. antibiotika 3. Insulin efter skema BG x 8 og Insuman rapid s.c. afhængig af BG. 4. Fast insulin Behandlingsforløb

23
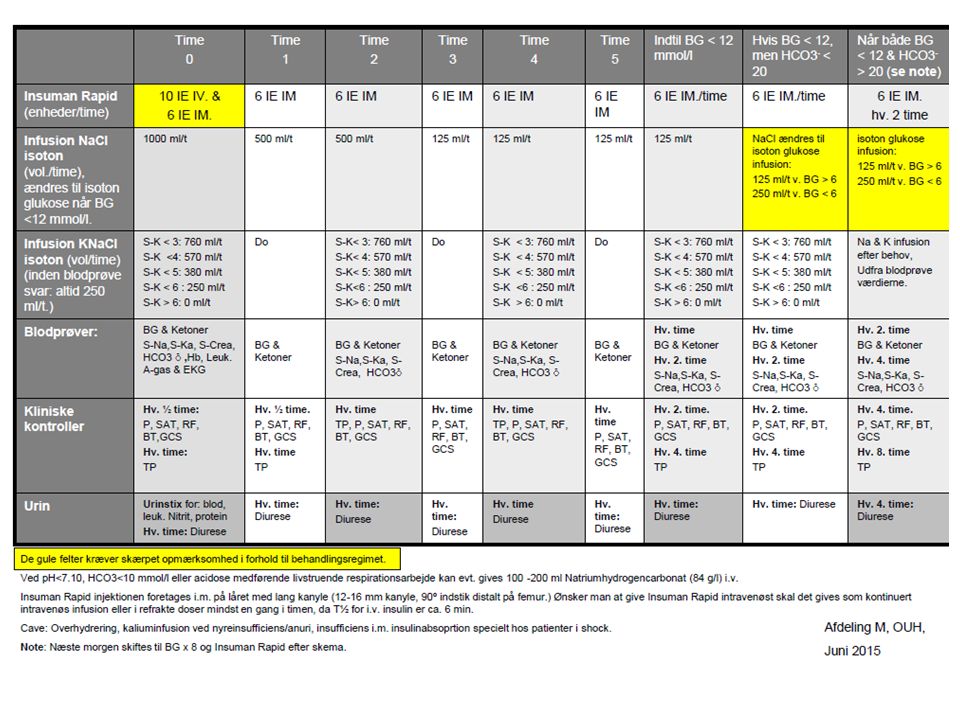
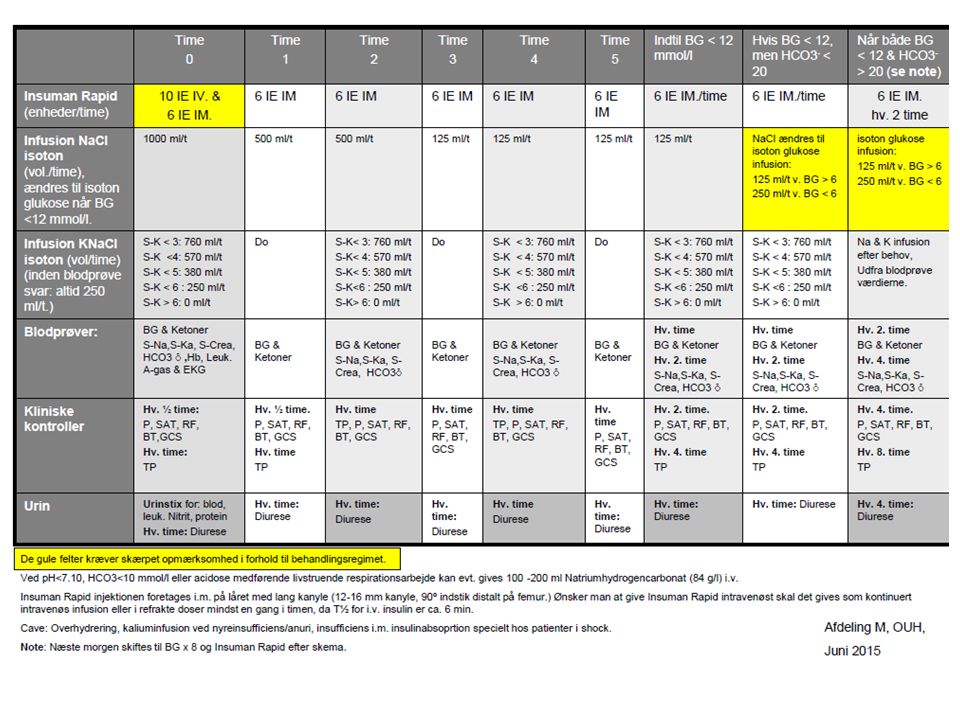
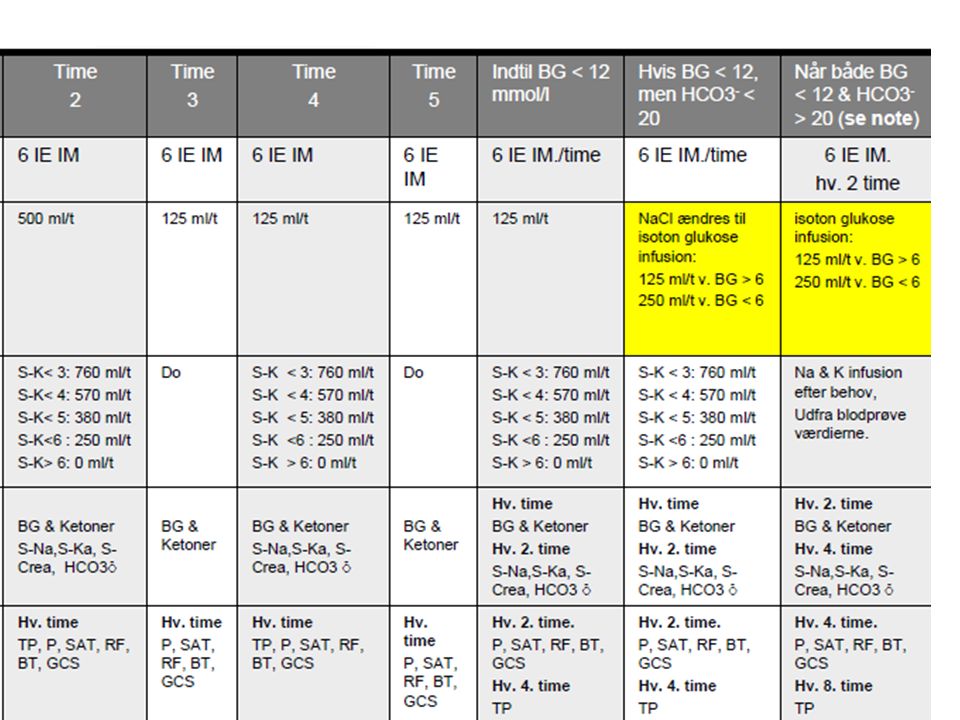
1. Ketoacidose regime 1. Insulin Straks Insuman Rapid 10 IE i.v. + 6 IE I.m. herefter 6 IE/time i.m., eller 6 IE/time i.v. (infusion/refrakte doser) 2. Væske og elektrolytter Mangler ved DKA: 5 - 8 liter vand 300 - 1000 mmol Kalium 400 - 700 mmol Natrium 3. Bicarbonat infusion (evt.) 4. Antibiotika (evt.)
 2. Væske og elektrolytter Mangler ved DKA: liter vand mmol Kalium mmol Natrium 3. Bicarbonat infusion (evt.) 4. Antibiotika (evt.).")
24
kalium

25
K+ = 3 - 5 mmol/l K+ = 140 - 150 mmol/l Na-K pumpe Stimuleres af insulin

29
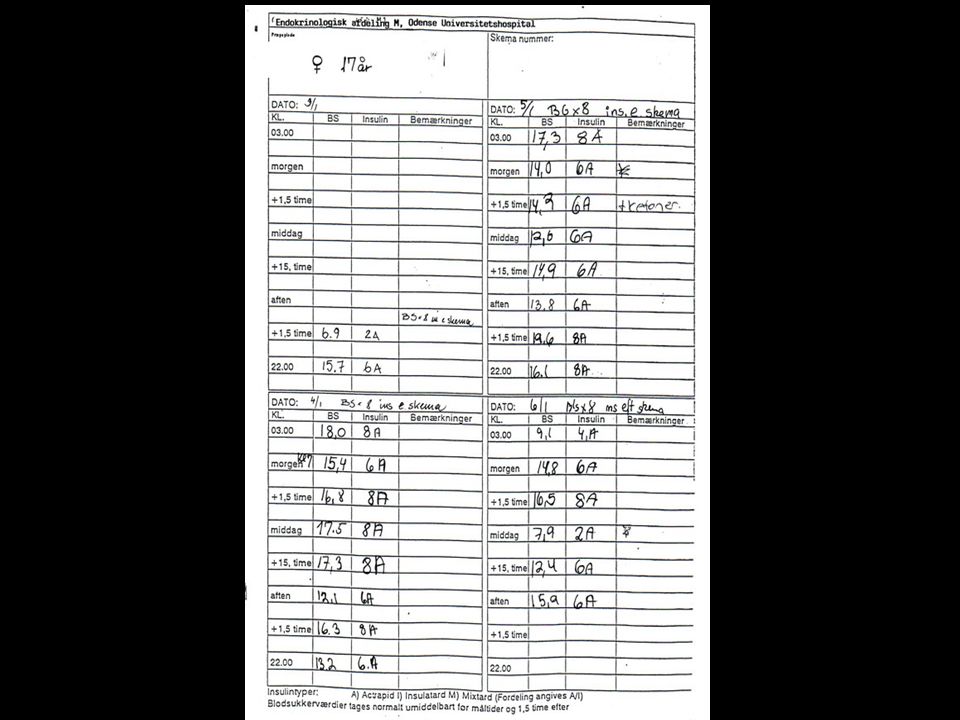
Diabetisk ketoacidose 1. Akut indlæggelse 2. Ketoacidose regime Insulin Væske og elektrolytter evt. bicarbonat evt. antibiotika 3. Insulin efter skema BG x 8 og Actrapid s.c. afhængig af BG. 4. Fast insulin Behandlingsforløb

30
B-glukose x 8, insulin efter skema Blodglukose måles før de 3 hovedmåltider og 1½ time efter, samt kl. 22 og kl. 03, og Insuman Rapid gives s.c. afhængig af den målte blodglukose værdi B-glukoseDosering 16 mmol/l Ingen insulin 2 IE Actrapid 4 IE Actrapid 6 IE Actrapid 8 IE Actrapid

32
B-glukose x 8, insulin efter skema Kan anvendes ved tilstande med et uafklaret insulinbehov eller ved vekslende insulinbehov, f.eks. ved: Nyopdaget diabetes (kun få dage) Efter fødsel (insulinbehov ”halveres”) Efter operation (”til pt atter spiser nornalt”) Akut interkurrent sygdom (”op-ned”)
 Efter fødsel (insulinbehov halveres ) Efter operation ( til pt atter spiser nornalt ) Akut interkurrent sygdom ( op-ned ).")
33
Diabetic Ketoacidosis (DKA) vs Hyperosmolar Hyperglycaemic State (HHS) (HONK)
 vs Hyperosmolar Hyperglycaemic State (HHS) (HONK)")
35
Kitabchi et al. Diabetes Care 2009; 32: 1335 52 mM 34 mM

36
”Euglycaemic” Ketoacidosis Estimated ~ 10% of DKA Definition: ketoacidosis with p-glucose < 250 mg/dl = 13.8 mM on admission, and p-bicarbonate < 10 mM -Exogenous insulin en route to to the hospital -Starvation, low-calorie intake, -Pregnancy, womiting -Inhibition of gluconeogenesis Diabetic Ketoacidosis (DKA) P-Glucose (mg/dl) >250 ~ (>13.8 mM) (oftest 30-40 mM) A-pH <7.30 (normal 7.35-7.45) S-Bicarbonate < 15 mEq/l B-Ketoner (hydroxybutyrat) > 3 mmol/l Urin-ketoner +++ ? (B-Ketoner normalt <0.6mM, faste 0.6-3.0mM, (Abbott: B-Ketoner 16mM OBS begyndende DKA)
.")
37
Case fra Kolding 40 årig kvinde, DM-1, HbA1c 79 mmol/mol, gravid i 12. uge, svær hyperemesis, 17.10. Kommer i svangreklinikken i Kolding stærkt forkvalmet, mavepine, ønsker ikke at spise eller drikke noget, får væske og Novorapid i refrakte doser. 18.10. 08.00 Flyttes til Akut afd. OBS stuen og startes DKA behandling (Urinstiks: 3+ glukose og 5+ ketoner, P-Glucose = 17,3, pH = 7,38, Hydrogenkarbonat = 15,1, Na = 137, K+ = 3,8, Cl- = 114 (normalt 98-108) Novorapid 10 IE i.v. og drop med 5 IE/time i.v. + i.v. væske: Isoton NaCl til max indløb, Isoton NaKCL 500ml/time Isoton glucose, GIK-drop (NaK-Glucose med 10 IE Novorapid). 19.10. Væskestatus. Indgift 14,8L, udgift 5,5L, balance +10,3L P-Glucose = 14,2, pH = 7,42, Hydrogenkarbonat = 15,7, Na = 121, K+ = 4,0, Cl- = 114
 Novorapid 10 IE i.v. og drop med 5 IE/time i.v. + i.v. væske: Isoton NaCl til max indløb, Isoton NaKCL 500ml/time Isoton glucose, GIK-drop (NaK-Glucose med 10 IE Novorapid) Væskestatus. Indgift 14,8L, udgift 5,5L, balance +10,3L P-Glucose = 14,2, pH = 7,42, Hydrogenkarbonat = 15,7, Na = 121, K+ = 4,0, Cl- = 114.")
38
Diabetic Ketoacidosis (DKA) P-Glucose (mg/dl) >250 ~ (>13.8 mM) (oftest 30-40 mM) A-pH <7.30 (normal 7.35-7.45) S-Bicarbonate < 15 - 18 mEq/l B-Ketoner (hydroxybutyrat) > 3 mmol/l Urin-ketoner +++ ? (B-Ketoner normalt <0.6mM, faste 0.6-3.0mM, (Abbott: B-Ketoner 16mM OBS begyndende DKA)
.")
39
SLUT

Lignende præsentationer